Electronic Disease Surveillance (EDS) System
Must-Have Capabilities, Modernization Best Practices, and Costs
In healthcare IT since 2005, ScienceSoft builds custom EDS platforms and focused epidemiological surveillance software modules for public health agencies that need cleaner reporting workflows, better interoperability, and surveillance tools aligned with local program and jurisdiction requirements.
 System - ScienceSoft")
Contributors

Head of AI, Principal Architect, ScienceSoft

Senior Solution Architect, Healthcare, ScienceSoft
The Fundamentals of Electronic Disease Surveillance Software
Electronic disease surveillance systems (EDSS) help public health agencies collect and validate reportable condition data, support case investigation and contact tracing, coordinate outbreak response, and produce the reporting required for public health action. Agencies usually choose custom software development when their existing EDS tools require excessive manual work, cannot be cleanly adapted to local workflows and reporting rules, or hamper interoperability.
Common EDS Implementation Scenarios
| Scenario | When ScienceSoft recommends it | What it looks like in practice |
|---|---|---|
|
Scenario
Focused EDS module |
When ScienceSoft recommends it
The agency already has core surveillance systems in place but still relies on manual handoffs, duplicate data entry, or disconnected reporting steps. |
What it looks like in practice
Adding a targeted module for condition intake, case investigation, outbreak management, reporting, public health communications, or another high-friction surveillance workflow. |
|
Scenario
EDSS modernization |
When ScienceSoft recommends it
The agency needs to improve or gradually replace a legacy EDSS without disrupting reporting, investigations, or connected systems. |
What it looks like in practice
Auditing the legacy EDSS, migrating and improving the quality of source data, redesigning outdated workflows, and updating ELR, eCR, or reporting interfaces. |
|
Scenario
Specialized EDS platform |
When ScienceSoft recommends it
The agency needs a dedicated surveillance system for a disease area, public health program, NGO initiative, or a smaller-scale surveillance environment. |
What it looks like in practice
Designing condition-specific forms and workflows, case investigation tools, core analytics, and the integrations needed to automate data exchange. |
|
Scenario
Comprehensive EDSS |
When ScienceSoft recommends it
The agency wants one primary environment for most surveillance functions across programs, teams, or jurisdictions. |
What it looks like in practice
Building a full-scale solution that supports end-to-end intake, investigation, contact tracing, outbreak management, intervention follow-up, analytics, national reporting, and broader interoperability. |
Implementation time: 4–12 months for a module or small-scale modernization; 10–18+ for a full-scale system or a large statewide modernization.
Development costs: $300,000–$2,000,000+ for a module or a focused, smaller-scale platform, with larger multi-year modernization programs estimated separately.
Must-Have EDS System Functionality
Our consultants outline the high-demand functionality typically expected by public health agencies. Depending on the agency’s actual workflows, modernization priorities, and surveillance scope, ScienceSoft can deliver any combination of the capabilities below as a focused module or a full-scale new system. Many of these processes can also be enhanced with AI assistants and agentic workflows.
![]()
Condition reporting
Reportable condition data may enter through electronic lab reporting (ELR), eCR/eICR, online forms, provider submissions, HIE feeds, or manual entry by public health staff. EDS intake workflows can then validate incoming reports, apply local reportability and routing rules, flag records for review, and launch condition-specific workflows. They can also process diverse laboratory message formats, handle result updates or corrections, and support onboarding of new conditions, labs, and reporting sources.
![]()
Recordkeeping
Epidemiologists and investigators can access linked case records, lab results, contacts, and identifiers for the same person, even when the data comes from different sources over time. An EDS system can preserve historical changes in demographics and identifiers, reduce duplicate records through automated matching and MPI-style identity resolution, and enable agencies to exchange governed data with external systems or other jurisdictions via standards-based interfaces and APIs.
![]()
Event detection
To identify potential outbreaks, unusual case clusters, or spikes in reportable conditions, surveillance teams can analyze data by geography, time period, syndrome group, and source. EDS systems help users compare new signals with existing records, recognize patterns that warrant follow-up, reclassify records as more information becomes available, and prioritize the items that should move to investigation first.
![]()
Case investigation
A case investigation workspace can bring together the details public health teams need to assess a report, document findings, and move the case forward. Within one flow, users may review investigation forms, add notes and attachments, capture demographics and exposure details, link lab results and identifiers, assign the record to an investigator, and update its classification or status as the picture becomes clearer.
![]()
Contact tracing
Investigators can trace transmission chains by linking exposed individuals to an index case, documenting person-to-person relationships, and tying interview and outreach activities to each contact. Risk factors, facility details, notes, and follow-up status remain attached to the contact record, which helps teams decide whom to prioritize and how exposure may have spread.
![]()
Outbreak management
During an outbreak, public health teams need one place to see how the situation is unfolding, which cases are already linked to it, and where follow-up is still pending. An outbreak management workspace can pull together confirmed and probable cases, related contacts, interviews, questionnaires, and response plans, while also helping teams track patterns by geography, setting, and time.
![]()
Intervention and follow-up management
Public health teams may need to tie next steps to a case or contact, check whether interventions were completed, and keep a record of the outcome over time. EDS platforms can support that work with disease-specific intervention plans, reminders, task tracking, and case-closure logic, helping agencies keep follow-up activities aligned with reporting requirements, intervention protocols, and operational deadlines.
![]()
Workflow configuration
Surveillance processes often vary by program area, condition, jurisdiction, and stage of investigation. EDS platforms can reflect that variation through configurable workflows that route records, assign next steps, trigger reminders, escalate overdue items, and apply business rules without hard-coding each process. Agencies may also configure alerts and notifications tied to deadlines, thresholds, status changes, or other events that require action.
![]()
Surveillance analytics
Dashboards, maps, queries, and scheduled reports give epidemiologists, investigators, and program managers different ways to work with the same surveillance data. EDSS platforms can support routine and ad hoc analysis, let users filter records by multiple parameters, drill down from trends to individual records, and export results for deeper review. They may also surface operational metrics alongside epidemiologic views such as charts, GIS-based visualizations, and trend summaries.
![]()
Public health communications
EDSS platforms may support public-facing and partner-facing communication workflows directly or through integrations with health alerting tools. On the intake side, agencies can use portals and configurable forms to collect reports, documents, and other submissions from providers, external partners, or the public, with validation and notification steps built into the process. On the outbound side, the same platforms may help teams send alerts, updates, and other public health communications to the right audiences using templates, recipient rules, and trigger-based workflows.
![]()
National and jurisdictional reporting
An EDSS can facilitate the preparation, submission, and tracking of reportable-condition data for local, state, territorial, federal, donor, or other program-specific reporting workflows. This may include support for required report formats, case notification logic, validation checks, acknowledgments, error handling, corrections, resubmissions, and exchange with peer public health systems or national authorities.
Not Sure How Much EDS You Actually Need?
ScienceSoft can help you assess your current surveillance environment, identify the highest-friction workflows, and define a realistic implementation scope.
How AI Capabilities Can Support Disease Surveillance
ScienceSoft helps public health agencies apply AI in EDS where it can reduce manual effort, speed up surveillance work, and improve consistency in data handling, investigation support, analytics, and public health communications.
To keep AI use safe, each capability can start as a tightly scoped module with clear data boundaries, auditability, and human review in workflows that affect investigation, reporting, or outward-facing communication. This approach works for both language models and traditional machine learning and makes it easier to validate results before scaling further.
![]()
Record intake and cleanup
AI assistants based on language models (LLMs and SLMs) can help intake teams and investigators clean up records before data issues spread through the EDSS. They can extract symptoms, dates, exposures, provider details, and other case elements from emails, PDFs, notes, scanned forms, or free-text reports, then suggest structured fields, code mappings, or likely corrections. They can also flag missing, conflicting, or duplicate information for staff review before the record moves further.
![]()
Record linkage and deduplication
The same person may enter an EDSS through different source systems and under different identifiers, names, or demographic details. ML-driven copilots can help surveillance teams and data stewards spot likely matches across lab reports, case records, contact records, and follow-up data, even when the fields do not line up perfectly. This improves longitudinal history, reduces duplicate records, and gives investigators a more complete record to review.
![]()
Event detection and prioritization
Traditional machine learning can help epidemiologists and surveillance teams spot unusual clusters, spikes, or other signals that deserve review. Built into an EDSS, such agents can scan data across time, geography, syndrome groups, and source systems, then rank alerts by likelihood or urgency. This helps staff focus on the records most worth investigating first, while still leaving final validation and escalation decisions to public health professionals.
![]()
Investigation copilots
Case investigations often involve long notes, fragmented updates, and details scattered across multiple records. Investigators and epidemiologists can use language model-based copilots to pull those pieces into a readable case summary, draft a timeline of events, and highlight facts such as exposure history, symptom onset, or follow-up actions. This can reduce the time spent reviewing text-heavy records and help staff prepare for case assessments faster.
![]()
Predictive surveillance analytics
Forecasting tools add a planning layer to EDSS reporting. Built on traditional machine learning, they can project near-term case volume for specific conditions, compare expected activity across regions, and surface trend changes that may not stand out in current reports yet. Epidemiologists and program managers can use these projections to adjust alert thresholds, prepare staffing, or investigate whether a developing cluster needs earlier attention.
![]()
Public health communications
Public health communication teams can use LLM or SML copilots to prepare draft alerts, public updates, provider notices, and FAQ-style responses faster. LLMs can adapt the same core message for different audiences, simplify technical wording, translate content, and suggest follow-up materials tied to a case surge or outbreak. Staff should still review every draft before release, especially when guidance is time-sensitive or jurisdiction-specific.
When introducing AI into EDS workflows, it helps to define early what level of automation is safe and actually useful. Low-risk tasks such as extraction, formatting, draft summarization, completeness checks, and alert ranking can often run automatically because they mainly prepare information for further review without directly impacting processes. By contrast, actions that alter case records, change workflow status, trigger reporting, or shape outward-facing messages should stay behind staff review and approval. I also recommend logging every step (source data, AI suggestions, confidence indicators, reviewer actions, and final updates), so the agency can validate performance, investigate errors, and maintain auditability as the use of AI expands.
Valuable Integrations for EDS Software
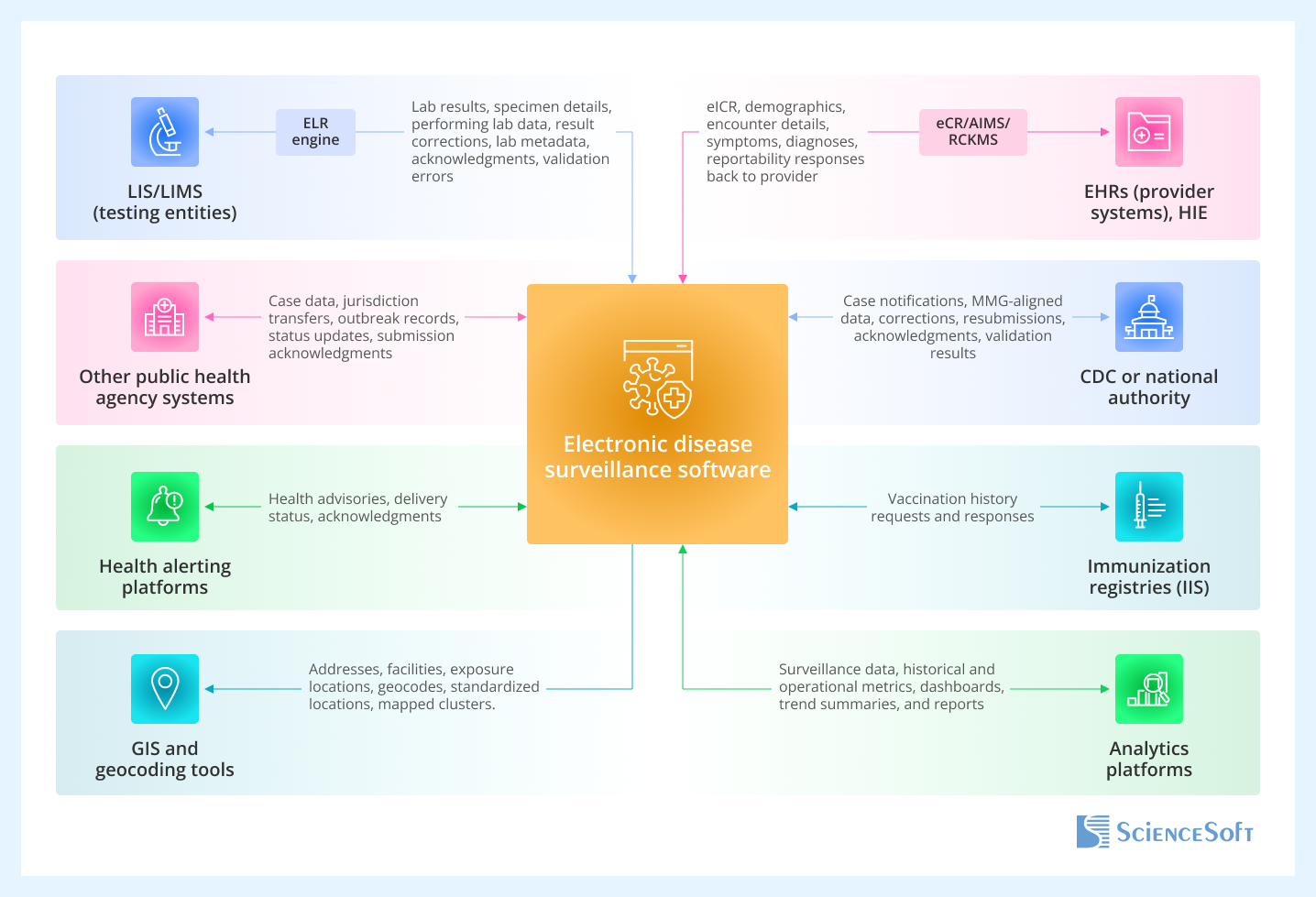
- Laboratory information systems (LIS/LIMS) of testing entities to automatically capture reportable lab results, link them to existing records, and launch condition-specific review workflows.
- EHRs (provider systems) and HIE to bring clinical context into surveillance records, including diagnoses, symptoms, encounter details, and provider-submitted case information.
- Public health agency systems to support cross-jurisdiction case exchange, reporting, and coordinated surveillance across local, state, and national programs.
- CDC or another national public health authority to exchange nationally reportable case data, support required submissions, and manage follow-up on reporting results.
- Health alerting platforms to distribute health advisories, outbreak notifications, and other urgent communications to providers, partners, or the public.
- Immunization registries to add vaccination history to case review and strengthen communicable disease follow-up.
- GIS and geocoding tools to visualize case locations, identify clusters, and support geographic analysis during outbreak investigation.
- Analytics platforms to power advanced epidemiologic reporting, trend analysis, and scheduled surveillance dashboards outside the core transactional workload.
Public Health Surveillance System Development Tips
![]()
Structure person, case, lab, and contact records separately — then link them
To make disease surveillance more reliable, it is better to keep the main EDSS record types separate but connected instead of forcing everything into one large case form. Person records, case records, lab results, and contact records do not change on the same timeline or serve the same purpose in surveillance workflows. Structuring them as linked records makes it easier for the software to preserve longitudinal history, manage multiple identifiers and lab results, support both person-centric and case-centric views, and reduce duplicate records without disrupting investigations.
![]()
Use established public health data exchange formats
When designing interoperability for a custom EDSS, it is usually safer to choose a small set of established public health formats and build the exchange layer around them:
- HL7 v2.x often makes sense for ELR and other long-standing public health messaging flows.
- FHIR works well for API-based exchange.
- eCR implementations should account for eICR, Reportability Response, and RCKMS/AIMS routing.
- CDC’s NNDSS message mapping guides (MMGs) are a practical reference for nationally notifiable case notifications.
This standard-first approach reduces the amount of custom translation logic you need to build and maintain. It also makes it easier to expand the EDSS later without having to redesign every new connection from scratch. Making custom data formats is still possible, but they work best as exceptions rather than the default.
![]()
Use current security and safe-use AI guidance as a design baseline
If you are looking for a reliable starting point for EDSS safeguards, it makes sense to anchor the design in a few current standards from the beginning. For example, NIST CSF 2.0 can frame the overall risk approach, NIST SP 800-53 Rev. 5 can guide the underlying security and privacy controls, and FIPS 140-3 can support cryptographic requirements where applicable. This gives you a structured way to define authentication, access control, encryption, audit logging, backup and recovery, and administrative safeguards before development moves too far. If the EDSS includes AI, CDC’s Considerations for Generative AI in Public Health is also worth using as implementation guidance, especially for data boundaries, human review, transparency, and governance.
![]()
Separate operational casework from analytics and reporting
An EDSS usually supports two very different types of work at once: day-to-day case handling and heavier reporting or analysis. Investigators and epidemiologists need fast access to records, while dashboards, maps, recurring reports, and ad hoc queries can place a much higher load on the data layer. Keeping those workloads separate helps protect operational performance, makes scheduled reporting easier to manage, and gives you more flexibility in how historical data is stored, archived, or prepared for analysis over time.
When agencies plan an EDSS initiative, one of the most important early decisions is what should be handled through configuration and what should require hard-coding. Public health workflows never remain static: reporting rules change, new conditions appear, questionnaires are revised, and thresholds or routing logic may need adjustment more than once a year. My rule of thumb: don’t hard-code what your staff will need to change routinely. Use configuration for the parts of the EDSS that are expected to evolve (forms, thresholds, routing rules, and condition-specific workflows) and reserve code updates for logic that is truly unique and unlikely to change often. The more you hard-code, the more expensive and risky change becomes later, because routine updates start turning into development work. Configuration, on the other hand, makes the platform easier to adapt, but only if you put clear governance around it. Otherwise, different teams may start changing core rules in different ways, leading to inconsistencies in workflows, case handling, and reporting.
Technologies We Use
Front-end programming languages
Languages
- HTML5
- CSS
- JavaScript
JavaScript frameworks
- Angular JS
- React JS
- MeteorJS
- Vue.js
- Next.js
- Ember.js
Mobile
- iOS
- Android
- Xamarin
- Apache Cordova
- Progressive Web Apps
- React Native
- Flutter
- Ionic
Low-code development
- Microsoft Power Apps
- Microsoft Power Automate
- App Engine Studio (ServiceNow)
- Bubble.io
Clouds
- Amazon Web Services
- Microsoft Azure
- Google Cloud Platform
- DigitalOcean
- Rackspace Technology
Platforms
- Microsoft Dynamics 365
- Salesforce
- Magento
- SharePoint
- ServiceNow
- SAP SE
DevOps
Containerization
- Docker
- Kubernetes
- Red Hat OpenShift
- Apache Mesos
Automation
- Ansible
- Puppet
- Chef
- Saltstack
- HashiCorp Terraform
- HashiCorp Packer
CI/CD tools
- AWS Developer Tools
- Azure DevOps
- Google Developer Tools
- GitLab CI/CD
- Jenkins
- TeamCity
Monitoring
- Zabbix
- Nagios
- Elasticsearch
- Prometheus
- Grafana
- Datadog
Databases / data storages
SQL
- Microsoft SQL Server
- Microsoft Fabric
- MySQL
- Azure SQL Database
- Oracle
- PostgreSQL
NoSQL
- Apache Cassandra
- Apache Hive
- Apache HBase
- Apache NiFi
- MongoDB
- Microsoft Fabric
Cloud databases, warehouses, and storage
AWS
- Amazon S3
- Amazon Redshift
- Amazon DynamoDB
- Amazon DocumentDB
- Amazon RDS
- Amazon ElastiCache
Azure
- Azure Data Lake
- Azure Blob Storage
- Azure Cosmos DB
- Azure SQL Database
- Azure Synapse Analytics
- Kinect DK
- Azure RTOS
Google Cloud Platform
- Google Cloud SQL
- Google Cloud Datastore
Other
- Microsoft Fabric
Generative AI
Models
- Large Language Models (LLMs)
- Small Language Models (SLMs)
- Multimodal models
- Computer vision models
- Image generation models
- ASR speech models
- TTS speech models
- Speech-to-Speech Models
- Audio models
- Real-time
Model adaptation and efficiency
- Training from scratch
- Data design
- Data labelling/annotation
- Fine-tuning
- Instruction tuning
- LoRA adapters
AI platforms and services
- Azure OpenAI Service
- Microsoft Foundry
- Amazon Bedrock
- Google Vertex AI
- Google AI Studio
- Hugging Face Inference
- Oracle Cloud
- G42/Core42
- NVIDIA AI Enterprise
Agents and orchestration
- RAG
- Graph RAG
- Agentic workflows
- OpenAI Agents SDK
- OpenAI Agents (platform/guides)
- AWS Agents
- Claude Agent SDK
- Google Agent Development Kit (ADK)
- Microsoft 365 Agents SDK (Copilot Studio)
- OpenClaw
- LangChain
- LangGraph
- smolagents
- LiveKit
- Dify
- n8n
- Faiss
- ChromaDB
- Qdrant
- Weaviate
- OpenSearch
- Pgvector
- Amazon Neptune
- Graph RAG Toolkit
- Neo4j
Healthcare-specific language models
- MedGemma
- MedLM
- BioMedLM
Traditional ML
Platforms and services
- Azure Cognitive Services
- Azure Machine Learning
- Microsoft Bot Framework
- Amazon SageMaker AI
- Amazon Transcribe
- Amazon Lex
- Amazon Polly
- Google Cloud AI Platform
- Google Vertex AI
Frameworks and libraries
- Apache Mahout
- Apache MXNet
- Caffe
- TensorFlow
- Keras
- Torch
- OpenCV
- Apache Spark MLlib
- Theano
- Scikit Learn
- Gensim
- SpaCy
ScienceSoft: An Experienced Partner for Public Health Software Development
- Since 2005 in healthcare software engineering.
- Mature quality management and security management systems backed by ISO 9001 and ISO 27001 certifications.
- Proficiency in achieving compliance with the requirements of HIPAA, GDPR, NIST, FIPS 140-3, CDC surveillance reporting, safe AI use for public health cases, and more.
- Hands-on experience with healthcare interoperability standards (HL7, FHIR, NNDSS MMG) and clinical coding vocabularies (e.g., ICD-10, SNOMED CT, LOINC, RxNorm).
- 9 principal architects to design secure software architectures that enable reliable data exchange and management across public health, clinical, and laboratory systems (including legacy solutions).
- In-house Project Management Office (PMO) to support predictable delivery, disciplined scope management, and controlled modernization of connected surveillance environments.
Certifications and awards
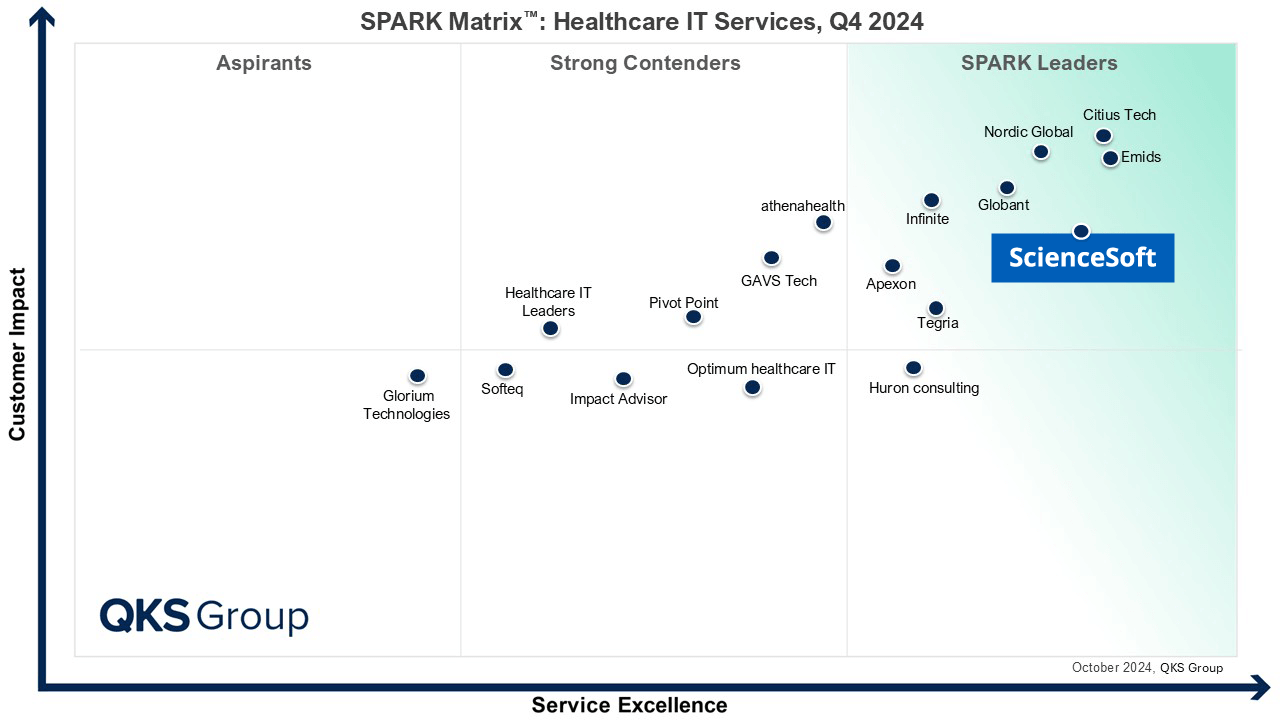
Featured among Healthcare IT Services Leaders in the 2022 and 2024 SPARK Matrix

Recognized for Healthcare Technology Leadership by Frost & Sullivan in 2023 and 2025
Named among America’s Fastest-Growing Companies by Financial Times, 5 years in a row

Four-time finalist across HTN Awards programs

Named among Becker’s Telehealth Companies to Know in 2026

Named Leading Healthcare Software Provider 2026 at Global Health & Pharma’s Healthcare & Pharmaceutical Awards

HIMSS Gold member advancing digital healthcare

ISO 13485-certified quality management system

ISO 27001-certified security management system
Development Costs of EDS Software
The costs of building a custom disease surveillance system range from $300,000 to $2,000,000+, depending largely on workflow scope, integrations, data migration needs, user groups, and compliance requirements. Large statewide modernization programs with broad legacy replacement, training, and multi-year support may exceed this range.
![]()
$300,000–$700,000
For a focused EDS module
We build a targeted module for a defined surveillance workflow, such as condition intake, case investigation, outbreak management, public health communications, or reporting and analytics. Projects in this range usually involve a limited user base, one core workflow, 1–2 integrations, and configuration around the agency’s reporting rules.
![]()
$800,000–$1,400,000
For EDSS modernization around a high-friction workflow
We modernize a specific part of an existing EDS environment without replacing the full system from day one. After the initial software assessment, the work may include data cleanup or partial migration, improvements to intake or investigation workflows, building configurable forms and routing rules, stronger reporting, and several integrations with lab, provider, public health, or analytics systems.
![]()
$1,500,000–$2,300,000
For a specialized EDS platform
We build a dedicated electronic disease surveillance system for a disease area, public health program, NGO initiative, or smaller surveillance environment. The functional scope may cover condition reporting, linked records, case investigation, configurable workflows, core analytics, and integrations with key external systems such as LIS/LIMS, EHRs, HIEs, IIS, GIS tools, or national reporting systems.
![]()
$2,400,000–$3,500,000+
For a broader EDS platform or phased modernization program
We build or modernize a larger EDSS environment designed to support multiple surveillance workflows, programs, or jurisdictions. The scope may extend to report intake, ELR/eCR-related flows, investigation, contact tracing, outbreak management, intervention follow-up, national reporting, advanced analytics, broader interoperability, and stronger governance.
Want a Custom Estimate for Your EDSS Initiative?
Tell us about your surveillance workflows, modernization plans, and integration needs, and ScienceSoft’s consultants will prepare a tailored project estimate at no cost.
