AI-Powered Healthcare Command Center
Capabilities, Architecture, Safety Guardrails
In AI engineering since 1989 and in healthcare IT since 2005, ScienceSoft builds healthcare AI solutions that close interoperability and workflow gaps across complex care environments. For healthcare command centers, we design and implement data, AI, and workflow components that turn live hospital data into operational decision support while meeting the constraints of existing hospital systems.

An AI-powered healthcare command center helps hospital teams manage patient flow, capacity, staffing, transfers, and discharge work from one coordinated operating layer. AI strengthens command centers by forecasting operational strain, explaining delays, prioritizing bottlenecks, and routing follow-up work to the right teams.
Custom healthcare command center software can align AI models, workflow rules, and integrations with the hospital’s service lines, capacity protocols, EHR, bed management, workforce management, transport, and transfer-center systems instead of adding AI as another disconnected dashboard.
How Artificial Intelligence Changes Healthcare Command Center Operations
Traditional healthcare command centers without AI already give hospitals a centralized way to monitor bed capacity, patient flow, staffing, and transfers. However, teams still need to interpret signals, identify patterns, decide on urgency, and coordinate work across departments.
AI adds an intelligence layer to this operating model:
- Traditional machine learning (ML) can surface issues that may be hard to recognize from live dashboards alone. Pattern detection and forecasting models identify constraints most likely to disrupt patient flow (e.g., discharge delays, staffing gaps, or rising admission pressure) and recommend the optimal ways to address them.
- Generative AI (typically, language models) can serve as a natural-language interface for staff, answering operational questions based on the data from connected systems, explaining the output of predictive models, or generating shift summaries.
- Agentic AI can help turn AI outputs into automated follow-up work that runs within strict workflow guardrails. For example, when the system predicts bed shortages in two units, an agentic workflow can check approved placement rules, pull the relevant capacity and staffing data, prepare recommended actions, and route tasks or escalation alerts to bed management, EVS, transport, or staffing teams for review.
The AI-enabled command center model is becoming increasingly justified in large hospitals and multi-hospital systems where the volume, variability, and interdependence of operational decisions make manual prioritization hard to sustain.
Benefits of AI Application in Healthcare Command Centers
![]()
Better use of existing capacity
Forecasting and prioritization can help hospitals unlock capacity that already exists but is hard to use due to delays, mismatches in placement, or slow coordination. Toronto's Humber River Hospital reported its AI-enabled command center could handle an 8% rise in average daily emergency department visits without adding staff or infrastructure, while also reducing inpatient waiting times and speeding up bed cleaning.
![]()
Fewer delays in patient movement
When AI supports placement, bed turnover, and escalation workflows, hospitals can reduce friction in day-to-day flow. Outcomes reported by Tampa General Hospital include 83% lower patient placement time, 28% fewer post-anesthesia care unit holds, 45% shorter bed-clean wait times, and 23% shorter waits from emergency department admission to an inpatient bed.
![]()
Stronger transfer and access performance
Earlier visibility into capacity and constraints can improve transfer acceptance and bed assignment. Johns Hopkins Medicine reported a 46% improvement in accepting complex transfers and 38% faster emergency department bed assignment after implementing its command-center model.
![]()
Less dependence on manual coordination
AI can move more work from calls, huddles, spreadsheets, and local workarounds into structured queues, ranked alerts, and guided follow-up workflows, giving operations teams a more stable way to manage complex hospital flows.
AI Capabilities for a Healthcare Command Center
AI can support a command center at different stages of healthcare operations: it can help predict operational strain, prioritize the most urgent issues, explain complex operational conditions, and orchestrate follow-up work across teams.
![]()
Capacity, demand, and staffing forecasting
An ML model can analyze current occupancy, ED arrivals, historical throughput patterns, and staffing rosters to forecast near-term operational load. These forecasts can support bed planning, staffing decisions, and surge management and appear in command center dashboards, planning views, and escalation routines.
![]()
Anomaly detection
A statistical ML model can monitor live operational signals and compare them with expected baselines for discharge pace, bed turnover, unit flow, etc. When unusual patterns appear, the system can flag them in monitoring dashboards and alert command center staff.
![]()
Digital twin simulation
A simulation engine with optimization models can create a digital representation of hospital operations using historical and live data. Teams can use it to plan and test different scenarios, such as opening surge beds or shifting procedure volume, before changing live workflows.
![]()
Network balancing
Forecasting and optimization models can compare projected demand and available capacity across hospitals, campuses, or service lines. This helps command center teams decide and coordinate where patients should be routed across the network.
![]()
Resource allocation recommendations
An optimization model can calculate and rank recommended options for using constrained resources such as beds, transport, or procedural slots under current and predicted demand. Rules-based logic can filter those options based on hard constraints, including staffing availability, bed type, and level-of-care requirements.
![]()
Alert triage and workflow orchestration
A classification model can identify which operational issues require action, rank them by urgency and likely impact, and route them to the appropriate workflow. A workflow agent can then trigger the next approved step, such as creating a task, escalating an unresolved issue, or reprioritizing follow-up work.
![]()
Conversational analytics
An LLM copilot with access to governed operational data can allow users to query live hospital conditions in natural language.The copilot can be embedded in a command center workspace, analytics portal, or executive dashboard. Staff can ask about delays, predicted occupancy, or pressure points without building a report or involving an analyst.
![]()
Automated operational summaries
A GenAI copilot can assemble structured summaries from live metrics, event feeds, and selected operational notes. This way, staff can review a draft summary instead of compiling updates manually from multiple systems. These summaries can be used during shift handoffs, operational meetings, and leadership briefings.
Essential AI safety and privacy guardrails
![]()
Human review and escalation
AI can prepare forecasts, rank alerts, or suggest next steps, but high-impact decisions stay with managers and coordinators. When model confidence is low, required data is missing, or hospital rules require oversight, the case is routed to the human staff with the relevant context attached.
![]()
Risk-based controls
Different AI use cases need different levels of control. Lower-risk uses, such as operational summaries, may need lighter review, while patient-specific recommendations, staffing changes, or actions that affect access to care require stricter validation, documentation, and approval.
![]()
Approved sources only
Generative AI features should be limited to approved sources, such as EHRs, ADT feeds, and operating playbooks. The language model retrieves facts from those sources and stays within defined task boundaries, rather than improvising actions or answers. When the available evidence is incomplete or conflicting, the workflow stops, requests more input, or escalates.
![]()
Role-based access
AI services can be configured so that each role sees only the data required for its task. For example, a staffing view may show shift coverage and forecast demand, while an operational summary may show throughput, predicted occupancy, and escalated issues. This helps enforce minimum-necessary data access and reduce unnecessary PHI exposure.
![]()
Clear explanations
For AI recommendations that affect placement, escalation, or resource use, the system should show the main factors behind the output. A reviewable rationale allows users to examine, question, confirm, or override the recommendation within the workflow, rather than relying on an opaque score or suggestion.
![]()
Model testing and monitoring
Before go-live, AI models should be tested against local workflows, historical data, edge cases, and relevant user groups. After deployment, hospitals should continue monitoring accuracy, false alerts, subgroup behavior, and performance drift as volumes, staffing patterns, or operational rules change.
![]()
Change control and audit logs
Model updates, workflow rules, and information sources are versioned and go through a controlled approval process for every change. The command center should also maintain logs of prompts, retrieved sources, model outputs, approvals, overrides, and downstream actions so teams can reconstruct how an output was produced and used.
How AI Works in a Healthcare Command Center
Below, ScienceSoft’s solution architects present a high-level reference architecture for AI in a healthcare command center. In this design, the command center sits above the hospital’s existing operational and clinical systems, which remain the systems of record. AI acts as an intelligence layer that interprets live hospital data, helps the command center predict strain, and routes selected outputs into copilots and workflow automation.
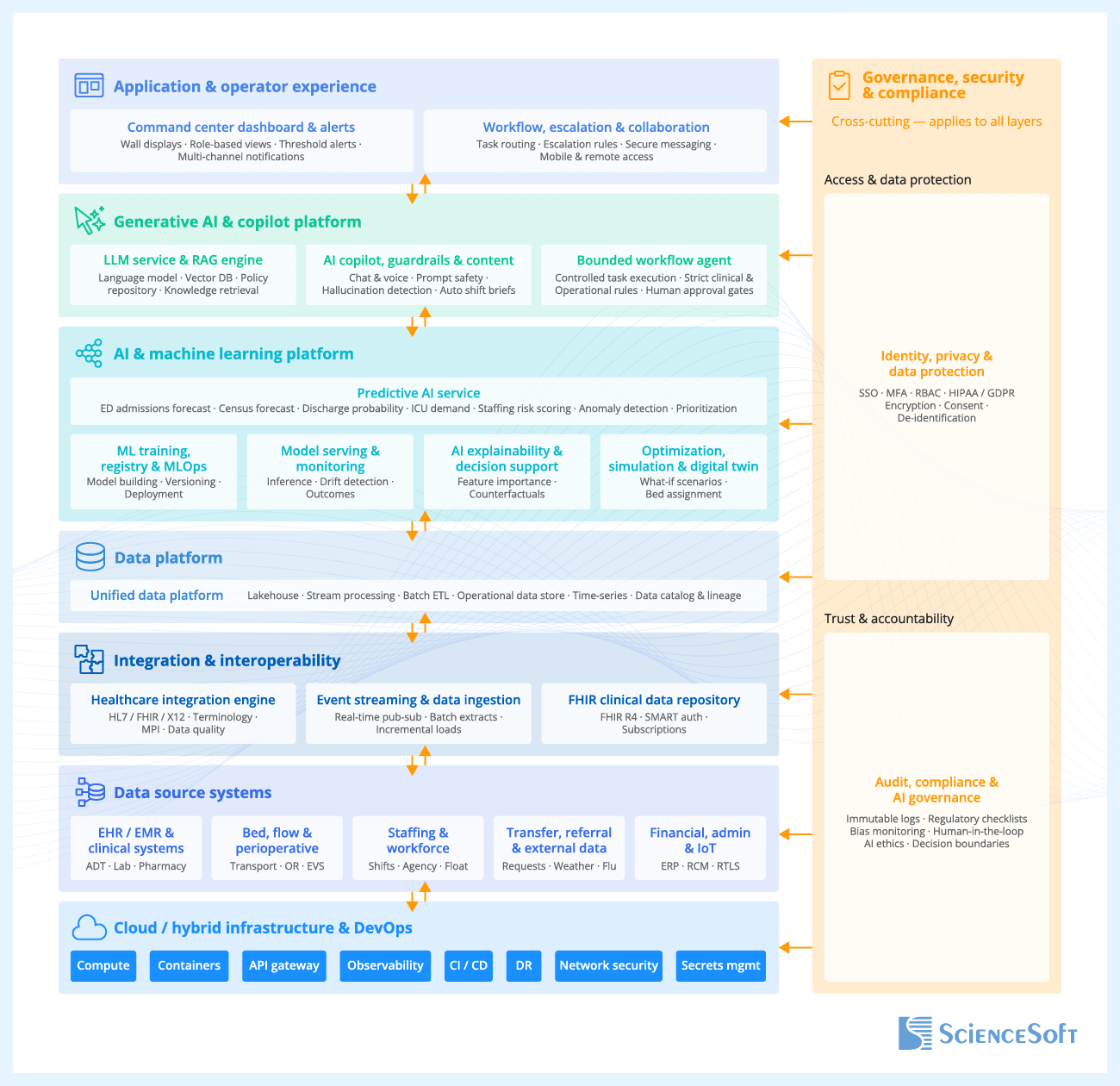
The main data inputs come from the EHR and ADT event feeds, hospital operations systems, and selected external sources such as weather feeds and public health alerts. These data feeds provide the inputs AI services need for forecasting, anomaly detection, and prioritization.
An integration engine translates, matches, and validates this data before it reaches AI components. It ingests HL7 v2, FHIR, APIs, and other source interfaces, matches patients, encounters, providers, and locations across systems, and standardizes fields such as bed status, unit assignment, and discharge state. For clinical data, the solution can use a FHIR repository as a normalized read model. It keeps a continuously refreshed, current-state view of the subset of patient data the command center needs, while the EHR and other source systems remain the systems of record. If a workflow needs to write back to a source system, the request goes through the integration engine, which translates it into the target format. The FHIR repository is updated only after the source system confirms the change.
The data platform is designed to support two technical workloads at once. One is live command center work, such as updating dashboards, sending alerts, and generating current predictions. The other is background work, such as comparing forecasts with actual outcomes and analyzing longer-term patterns. Keeping these workloads separate prevents heavy background analysis from slowing down the screens and alerts that staff rely on in daily operations.
The AI and ML platform includes the predictive AI service, which produces the forecasts, anomaly detections, risk scores, and priority rankings. These outputs appear in dashboards and alerts, feed the copilot with the data it needs to explain a forecast or a flagged issue, and can also trigger workflow rules that route specific issues to the right operational queue, such as the staffing office, bed management team, or transfer center. The platform also includes several supporting components: model training, registry and ML ops for model building and versioning, model serving and monitoring for running and tracking models in production, and AI explainability and decision support for showing what is driving a prediction or recommendation in a form staff can review. Where needed, the same platform can also include optimization, simulation, and digital twin components for what-if analysis and operational scenario testing.
The generative AI and copilot platform adds a natural-language interface on top of the predictive services. Its retrieval augmented generation engine grounds policy- and playbook-based responses in approved documents, while live operational facts can come directly from governed APIs, FHIR queries, or operational data stores. This helps the copilot answer from approved and current sources rather than from general model knowledge. Based on this approved content and analytics results, the copilot can answer user questions, create document summaries, or interpret analytics results.
If the solution includes a workflow agent (agentic AI), it acts through the workflow, escalation and collaboration module, using rules, escalation paths, and approval settings configured in the solution rather than acting on hospital systems directly.
The user-facing layer (application and operator experience) is where command center staff interact with AI. It surfaces predictions and alerts in dashboards and task queues and supports escalation and team coordination. Rather than appearing as a separate application, the copilot is built into the same command center interface for questions, explanations, and draft summaries.
Tech Stack for AI-Enabled Command Centers
Since 2005 in medical software engineering, ScienceSoft recommends using the following technologies for AI-enabled command center software development:
Generative AI
Models
- Large Language Models (LLMs)
- Small Language Models (SLMs)
- Multimodal models
- Computer vision models
- Image generation models
- ASR speech models
- TTS speech models
- Speech-to-Speech Models
- Audio models
- Realtime
Model adaptation and efficiency
- Training from scratch
- Data design
- Data labelling/annotation
- Fine-tuning
- Instruction tuning
- LoRA adapters
AI platforms and services
- Azure OpenAI Service
- Microsoft Foundry
- Amazon Bedrock
- Google Vertex AI
- Google AI Studio
- Hugging Face Inference
- Oracle Cloud
- G42/Core42
- NVIDIA AI Enterprise
Agents and orchestration
- RAG
- Graph RAG
- Agentic workflows
- OpenAI Agents SDK
- OpenAI Agents (platform/guides)
- AWS Agents
- Claude Agent SDK
- Google Agent Development Kit (ADK)
- Microsoft 365 Agents SDK (Copilot Studio)
- OpenClaw
- LangChain
- LangGraph
- smolagents
- LiveKit
- Dify
- n8n
- Faiss
- ChromaDB
- Qdrant
- Weaviate
- OpenSearch
- Pgvector
- Amazon Neptune
- Graph RAG Toolkit
- Neo4j
Healthcare-specific language models
- MedGemma
- MedLM
- BioMedLM
Traditional ML
Platforms and services
- Azure Cognitive Services
- Azure Machine Learning
- Microsoft Bot Framework
- Amazon SageMaker AI
- Amazon Transcribe
- Amazon Lex
- Amazon Polly
- Google Cloud AI Platform
- Google Vertex AI
Frameworks and libraries
- Apache Mahout
- Apache MXNet
- Caffe
- TensorFlow
- Keras
- Torch
- OpenCV
- Apache Spark MLlib
- Theano
- Scikit Learn
- Gensim
- SpaCy
Healthcare interoperability
- HL7 v2
- FHIR
- SMART on FHIR
- Azure Health Data Services
- Amazon HealthLake
- Google Cloud Healthcare API
Data platform
- Azure Data Lake
- Amazon S3
- Google Cloud Storage
- Snowflake
- Databricks
- PostgreSQL
- Apache Kafka
- Apache Spark
Data integration and processing
- Azure Data Factory
- Apache Airflow
- Apache Kafka
- Apache Spark
Analytics and reporting
- Power BI
- Tableau
Real-Life Examples of Artificial Intelligence Application in Healthcare Command Centers
|
|
Children’s Mercy Kansas City launched a Patient Progression Hub that uses predictive analytics and real-time operational data to manage patient flow from admission request to discharge. Within six months, the hub created additional bed capacity for 82 medical-surgical patients annually, reduced bed-related deferrals to zero during the winter surge, and almost eliminated ED boarding. |
|
|
Tampa General Hospital expanded its care coordination platform with an artificial intelligence layer built on real-time hospital data and large language models. The health system reported an 83% reduction in the time required to place patients, a 28% decline in PACU holds, and a 30% reduction in mean length of stay for sepsis patients after earlier AI-powered workflow deployments. |
|
|
Duke Health is using an AI-powered command center to turn complex hospital data into actionable operational insight. The system is reported to have achieved a 6% productivity boost, 66% faster bed assignment, a 50% reduction in temporary labor use, and capacity for 500 additional patients annually. |

Hospitals do not need to modernize every legacy system before introducing AI into a command center. In many projects, AI is added around existing operational systems; integration, data quality, and interoperability issues are addressed as part of the implementation.
Success usually depends less on having a perfect technology landscape and more on starting with the right operational data. The first priority is not even all hospital data, but the core data streams for the first AI use cases (e.g., if the goal is occupancy forecasting, the most important data would be admissions, discharges, transfers, bed status, and staffing). Those data inputs need to arrive on time, use the same event definitions across systems, and pass validation before they are used for predictions or alerts.
Challenges of AI in Healthcare Command Centers We Solve
![]()
Challenge 1. Hospital data is too fragmented for reliable AI output
In many hospitals, one event can be recorded differently across systems, as these systems often use different identifiers, status values, and update cycles. Staff can often work around these differences in dashboards, but AI is less tolerant. When source records do not match, predictions, prioritization, and automation become less dependable.
Solution
![]()
Challenge 2. Models lose accuracy as hospital conditions change
Predictive models do not stay reliable automatically. Changes in referral volume, staffing patterns, discharge practices, case mix, or seasonal demand can make a previously accurate model less useful for current command center decisions.
Solution
![]()
Challenge 3. GenAI and agentic workflows can produce unsupported or out-of-policy actions
In a healthcare command center, a copilot may answer questions, summarize live conditions, or draft updates, while a workflow agent may create tasks or trigger escalations. Without strong controls, these components can rely on outdated policies, use incomplete context, or act outside approved operating rules.
Solution
How Much Does It Cost to Add AI to a Healthcare Command Center?
When determining the cost of implementing AI into command centers, ScienceSoft considers the following factors:
- The number of facilities and workflows in scope.
- The number of source systems to connect.
- The amount of data mapping and validation required.
- Whether AI only informs decisions or also drives tasks and writeback.
- Whether the scope includes predictive AI only or also GenAI.
- The depth of governance, audit, security, and monitoring controls.
The cost of implementing an AI-powered healthcare command center solution usually ranges from $120,000 to $650,000 for an AI add-on or pilot covering one workflow on top of existing systems. A broader software layer that covers multiple workflows typically moves into the $700,000–$2,000,000 range. Multi-hospital programs with many source systems, writeback automation, physical command center setup, or major command center process redesign require a separate estimate and may exceed this range.
This estimate covers software development, the adaptation of market-available AI models, integration with existing hospital systems, data preparation, dashboard or copilot embedding, and model monitoring setup. Ongoing infrastructure and model licensing costs are not included.

Need to understand the budget for your project?
Why Trust Your AI Initiative to ScienceSoft
- In healthcare IT since 2005.
- In data analytics, data science, and AI since 1989.
- 150+ completed healthcare projects across clinical and administrative workflows.
- AI consultants and developers with 7–20 years of relevant experience and competencies in major ML technologies, frameworks, and libraries.
- Hands-on experience in implementing healthcare AI solutions for operational workflows and staff support, including call center automation and chatbots.
- Expertise in HIPAA, GDPR, PDPL, FDA, ONC, and other healthcare regulatory requirements.
- Proficiency in healthcare interoperability standards, including HL7 v2, FHIR, SMART on FHIR, and USCDI, as well as clinical terminologies such as ICD-10, SNOMED CT, LOINC, and CPT when clinical data is used.
- Ready to sign a BAA (Business Associate Agreement).
Certifications and awards
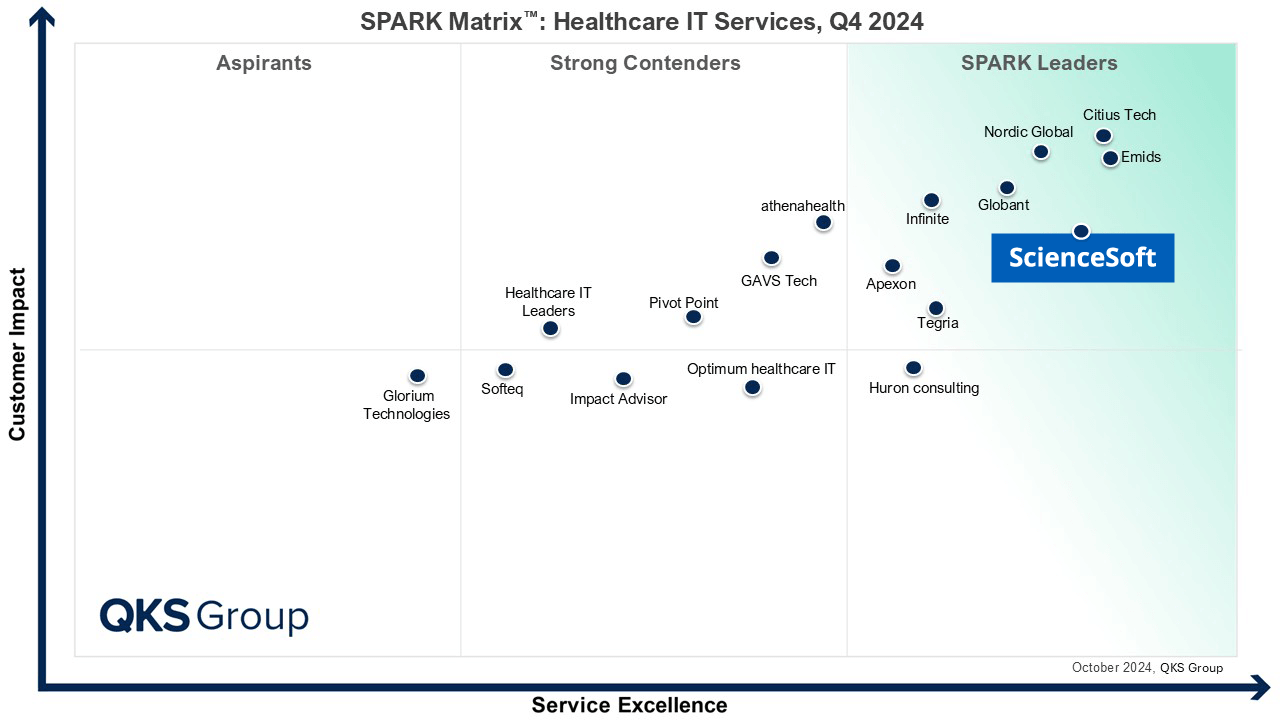
Featured among Healthcare IT Services Leaders in the 2022 and 2024 SPARK Matrix

Recognized for Healthcare Technology Leadership by Frost & Sullivan in 2023 and 2025
Named among America’s Fastest-Growing Companies by Financial Times, 5 years in a row

Four-time finalist across HTN Awards programs

Named among Becker’s Telehealth Companies to Know in 2026

Named Leading Healthcare Software Provider 2026 at Global Health & Pharma’s Healthcare & Pharmaceutical Awards

HIMSS Gold member advancing digital healthcare

ISO 13485-certified quality management system

ISO 27001-certified security management system
Our Clients Say

They collaborated with our medical professionals with great professionalism and care <…>. We found ScienceSoft to be dependable and forward-thinking, and we would confidently recommend them for high-responsibility projects.
Todd Nilson
MD
We are thankful for the meticulous and value-driven approach of ScienceSoft’s team. ScienceSoft’s project manager, business analyst, QA and software engineers were always friendly and ready to answer our questions or solve any ad-hoc issues.

ScienceSoft has been a competent partner for medical software development. We would recommend them as a trustworthy vendor. They are reliable, thorough, smart, available, extremely good communicators and very friendly.

Working with ScienceSoft was nothing but a learning experience <…>. They’re very responsive and very knowledgeable. I recommend ScienceSoft for any needs and will work with the company again if needed in the future!