Cardiovascular Information Systems (CVIS)
Functionality, Integrations, and Costs
In healthcare software engineering since 2005, ScienceSoft builds CVIS solutions that boost study reader throughput, ensure consistency of reporting, and meet physicians’ expectations for performance and usability. We design integration-first systems that work seamlessly with enterprise EHR, PACS, and device fleet and support data submission to cardiology registries.
 - ScienceSoft")
Contributors

Head of AI, Principal Architect, ScienceSoft

Senior Healthcare IT & AI Consultant, ScienceSoft
CVIS Overview
Cardiovascular information systems (CVIS) centralize key cardiology workflows, from test orders and scheduling to study interpretation and result sharing. A modern CVIS should support multi-modality imaging (echo, vascular, nuclear, CT, and MR studies), test result reporting with auto-populated measurements, ECG acquisition, hemodynamics data capture, and submission of registry-ready data for ACC programs with tight EHR and PACS integration.
ScienceSoft implements full-scale custom CVIS solutions and targeted CVIS modules or extensions for cardiovascular providers who find out-of-the-box CVIS options insufficient for their workflows.
- Ambulatory cardiology physician groups (independent or system-owned) commission lean echo and ECG domains embedded into their EHR to centralize echo reading and ECG over-read across sites. This way, they avoid implementing a costly hospital-oriented vendor CVIS that would sit outside their EHR workflows.
- Specialty cardiac hospitals commission targeted CVIS extensions that normalize structured reporting, automate NCDR/TVT registries, or tighten implant charging where their standard CVIS leaves gaps. Some cardiac hospitals also choose to replace their cardiology stack with a full-scale custom CVIS platform when their existing CVIS fails to provide service-line-wide governance and analytics.
- Medical centers and integrated delivery networks with cardiovascular service lines may deploy a custom CVIS governance layer on top of existing PACS and departmental CVIS to standardize templates, registries, and KPIs. It unifies governance, which vendor CVIS packages often fail to do.
Implementation time: 6–12+ months for a CVIS extension and 18–24+ months to engineer a full-scale CVIS.
Development costs: from $250,000 for a basic CVIS extension pack, which enhances structured reporting, registry dataset validation, and viewer performance, to $3,500,000+ for an advanced full-scale CVIS platform with an invasive cardiology module and AI automation. Use our free calculator to get a tailored estimate for your project.
Essential and Advanced Capabilities of a Cardiovascular Information System (CVIS)
Below, ScienceSoft’s consultants share a comprehensive map of CVIS capabilities that reflects the needs we most often see across our cardiology clients. In real-world projects, providers typically select and phase in only the modules that match their clinical priorities and budget to control TCO and ensure a clear payback.
Clinical workflows
![]()
Clinical workspace for multi-modality cardiac imaging
- Unified cross-site worklist receives study orders from EHR, organizes image reading queues by priority, and assigns readers.
- Enterprise-wide web viewer streams ultrasound, nuclear, CT, MR, and interventional images from connected imaging systems for zero-footprint review.
- Reader workspace provides role-based tools for cine image review, manual measurements, annotations, and configurable hanging protocols per modality.
- Multi-monitor reader layouts support auto-fetching of prior exams and side-by-side comparison with the current study.
- Single sign-on launch from the EHR opens the correct patient and study directly in the viewer.
Value-adding features
-
Waveform-enabled viewer shows ECG or hemodynamic traces alongside echo, CT, MR, or angiography images for synchronized waveform–image review.
- Patient-centric timelines list all cardiology exams and reports chronologically, with drill-down to images and detailed report content.
![]()
Image quantification and procedural planning add-ons
- Automated echocardiography strain analysis module identifies standard views, places contours, and outputs reproducible GLS measures under full physician edit control.
- CT or MR quantification workspace applies protocol presets for study types and standardizes ventricular and myocardial measurements with labeled anatomical landmarks.
- Nuclear quantification toolkit calculates predefined perfusion and function metrics for SPECT, PET, and hybrid CT studies for reporting.
- Quantification rule engine checks required measurements and value ranges before report sign-off and flags missing or inconsistent data.
- CT- or MR-based procedural planning workspace captures measurements, writes results into reports, and assembles packets for structural and coronary interventions.
Value-adding features
- Vendor-neutral quantification integration unifies ultrasound, nuclear, CT, and MR tools in a single workspace, with consistent measurement names and units.
![]()
Structured reporting for multi-modality cardiac imaging
- Unified report templates define protocol-specific fields for echocardiography, vascular, nuclear, CT, MR, and interventional cardiology with registry-ready structures.
- Report template editor enforces controlled dictionaries, mandatory sections, and version control for consistent terminology and structure across locations.
- Auto-fill engine populates numeric and categorical report fields from imaging, monitoring systems, and measurements created in the CVIS viewer.
- Report finalization workflow supports editing findings, adding comparison narratives, selecting key images, and completing sign-off.
- Report distribution engine sends finalized reports with key images to the EHR, patient-ready portal views, and external referrers.
Value-adding features
- Report validation rules check required fields and measurement consistency before sign-off and display issues for correction.
- Cross-vendor measurement mapping standardizes units and labels from different devices and sites.
![]()
ECG management
- Unified SCP-ECG and DICOM waveform ingestion pipeline consolidates data from ECG carts, Holter, telemetry, and monitoring systems into a searchable repository.
- Stress ECG protocol capture module records testing stages, workload, vitals, and recovery times as discrete data fields in the ECG report.
- Rules-based ECG triage flags studies with abnormal device measurements and prioritizes them for cardiologist review.
- Browser-based ECG review workspace displays current and prior waveforms with calipers and supports interpretation and sign-off in one UI.
Value-adding features
- ECG cart worklist with wristband scanning pulls EHR orders and auto-populates patient demographics at the bedside.
- ECG normalization and archival gateway converts SCP-ECG into DICOM waveforms for long-term VNA storage.
![]()
Hemodynamics and intraprocedural data capture
- Real-time hemodynamics capture tool records pressure and flow traces by procedure type, runs protocol-defined calculations, and stores results with synchronized timestamps.
- Procedure event log records medication and contrast administration, device usage, and complication events in chronological order, synced with images and vital signs.
- Automated data transfer service feeds captured values and events into reports and the cardiology procedure log.
Value-adding features
- Multi-lab connectivity with local caching and HL7, DICOM, and XML interfaces keeps hemodynamic data synchronized across procedure rooms.
- Time-aligned workflow enforces enterprise clock synchronization across imaging, monitoring, and reporting systems.
- Touch-optimized intraprocedural UI presents large control elements for quick event entry on procedure room panels and tablets.
![]()
Cardiology registry and quality reporting (for NCDR and TVT)
- Versioned registry dictionaries and field mappings keep CVIS structured report fields aligned with current NCDR and TVT data elements.
- Registry dataset generation and validation workflow auto-fills registry fields from CVIS reports, runs ACC completeness checks, and flags data defects.
- Review worklists with source links route missing or conflicting fields to reviewers and open the relevant study, image, or report.
- Submission engine compiles validated datasets into harvest files, supports their uploads via ACC/NCDR portals, and returns submission status to reviewer queues.
Value-adding features
- NLP-assisted abstraction service prepopulates frequent registry fields from EHR notes and routes low-confidence items to reviewer queues.
- NCDR benchmark and TVT outcome import module loads feedback reports, populates NCDR’s peer quartiles or TVT’s outcomes, and feeds registry quality dashboards.
Service-line management
![]()
Operational analytics and service line management
- Leader worklists for load balancing combine scheduled and in-progress studies by reader and room and support reassignment across sites.
- Capacity and utilization view merges schedule data and exam status by room and shift, and highlights open and overloaded slots.
- KPI dashboards and scheduled reports display turnaround time, throughput, room utilization, backlog, and reader productivity using harmonized definitions across sites.
- Target KPI breach alerts notify leaders when turnaround or backlog thresholds are violated and point to the queues that require immediate action.
- Data-quality worklists surface studies with missing event timestamps or inconsistent status, with direct links to the source CVIS or EHR record.
Value-adding features
- Door-to-balloon component timers track time to first ECG, team call, patient arrival, arterial puncture, and balloon inflation in the catheterization lab.
- Reader productivity heatmap visualizes cases per hour and case mix by reader and location for staffing and workload planning.
- Cross-system data harmonization layer joins CVIS data with ADT and hemodynamic events for consistent multi-site analytics.
![]()
Implant traceability and charge accuracy
- Point-of-use barcode scanning captures device UDI, lot, and serial numbers into the patient chart and report, and into billing records for charge calculation.
- Real-time inventory decrement updates item quantities and locations in ERP and EHR to maintain par levels and prevent stockouts.
- Charge reconciliation dashboard validates charges against documented device and supply usage before claim submission.
- Implant recall management tool matches FDA recall notices to patient and stock records and tracks notifications and other follow-up actions for audit-ready compliance.
Value-adding features
-
Consignment and serial controls manage vendor-owned stock, provide proof of use, and support site-level reconciliation.
- Contract-aware price validation checks billed amounts against the item-master contract terms and expected discounts.
AI in CVIS: High-Impact Use Cases
ScienceSoft embeds explainable, controlled AI modules into CVIS solutions to reduce reporting burden, boost cardiology lab throughput, and cut avoidable invasive tests without forcing clinicians to leave their enterprise EHR (e.g., Epic or Oracle Health). All AI outputs stay limited to transparent, audited suggestions protected by operational guardrails at every step, so cardiologists retain full decision-making authority.
Below are the high-impact use cases, with their clinical and operational benefits confirmed by both ScienceSoft’s clients and independent sources.
![]()
AI-assisted echocardiography
- AI-guided view acquisition with on-screen prompts and automatic capture of required echocardiography views.
- Automatic view recognition and contouring, including apical view detection, endocardial borders placement, and speckle tracking to prefill GLS measurements.
- Prefilling CVIS echocardiography report templates with physician-validated measurements.
Reported benefits: GLS measurement time cut by ~60%; reduced user-related variability.
![]()
AI-driven ECG triage for low ejection fraction
- Low ejection fraction risk scoring on routine 12-lead ECGs, flagging likely low-EF cases with calibrated scores for cardiology follow-up.
- Triggering reflex tests (e.g., echocardiography, cardiology consults, or other standardized downstream steps) for high-risk patients.
- Context-aware ECG result presentation in EHR views with flags and links to representative abnormal waveform segments.
Reported benefits: higher diagnostic yield without added echocardiography volume with 34.2% predictive value; cost-effectiveness in outpatient settings.
![]()
AI-assisted coronary CT
- Lesion-level FFR-CT mapping engine computes noninvasive fractional flow reserve (FFR) values along coronary vessels for functional stenosis assessment.
- Co-registered FFR-CT visualization overlays color-coded FFR values and confidence scores on coronary CT images for review.
- FFR-based clinical triage rules support decisions on medical therapy, invasive angiography, or revascularization for coronary lesions.
Reported benefits: threefold shorter procedure time and similar diagnostic accuracy compared to invasive FFR; ~61% fewer invasive angiographies needed.
![]()
Predictive hemodynamic management
- Predictive hypotension alerting engine scores near-term risk from arterial pressure waveforms to prompt earlier correction.
- Protocol-aware treatment guidance module suggests fluid and vasoactive dose adjustments according to site-specific protocols.
- Episode-to-report prefill service summarizes hypotensive episodes and interventions into structured entries in EHR and CVIS.
Reported benefits: 41% shorter ICU length of stay; up to a 75% reduction of intraoperative hypotension time.
![]()
AI-powered cardiology registry (NCDR) data capture
- NCDR field prefill tool extracts values from EHR notes and CVIS data and populates registry fields with confidence and coverage scores.
- Source-linked provenance layer links each suggestion to its source sentence or measurement.
- Reviewer queues with model self-learning route low-confidence items for human validation and feed corrections back to models.
Reported benefits: a ~50% reduction in registry abstraction time & cost and 98–99% inter-rater reliability (ACC).
Whether ScienceSoft develops proprietary AI modules or embeds approved third-party models into CVIS, providers still work within the same core regulatory guardrails: HIPAA or GDPR privacy safeguards, Cures Act EHI access requirements, and, where applicable, ONC HTI-1 Decision Support Interventions transparency and FDA Clinical Decision Support expectations.
We focus on building the AI integration layer with access controls, data minimization, audit trails, and clear on-screen AI disclosures aligned with recognized risk management frameworks such as the NIST AI RMF. This approach helps our clients reuse the AI vendors’ regulatory documentation and keep the additional compliance effort as light as possible.

Planning a CVIS Initiative? Let’s Shape the Smartest Path Together
Essential Integrations for Cardiovascular Information System
ScienceSoft recommends planning CVIS integrations up front: failing to do this early often affects software delivery speed, clinician adoption, and long-term support costs. Here are the three main decisions you will need to make:
1. Which standard data exchange protocols, versions, and identifiers should all connected systems use so that EHR, PACS/VNA, or device upgrades don’t break integrations?
The best practice is usually:
- HL7 v2 and/or FHIR for test orders, reports, and APIs.
- DICOM for images and waveforms, DICOMweb for their web viewing.
- Standard medical code sets, such as LOINC or SNOMED, for consistent analytics.
- SSO via SAML or OAuth2/OIDC, preferably SMART-on-FHIR compatible, for authorization.
2. Should clinicians access CVIS via an embedded view in the EHR or via a new-window CVIS launch?
- EHR-embedded CVIS keeps clinicians in a single UI, preserves patient and study context, shortens training, and boosts adoption, but at the cost of tighter viewer and security constraints and closer alignment with the EHR release cadence.
- New-window CVIS launch decouples EHR and CVIS upgrades and enables complex multi-monitor layouts, but demands strict patient context management.
3. Should CVIS run under enterprise imaging (enterprise PACS, VNA, and a universal viewer) or as a standalone departmental CVIS?
- Enterprise imaging CVIS (within enterprise PACS, VNA, and universal viewer) centralizes lifecycle controls for prior exams and studies, eases cross-service access, and consolidates storage and licensing under a single governance model. However, it slows cardiology feature velocity and ties releases to enterprise roadmaps and standards.
- Departmental CVIS accelerates cardiology-specific UX and structured-reporting changes, and allows the service line to control upgrades. At the same time, it risks creating a new silo, duplicate storage, and inconsistent priors unless you define hard rules for handoff to the enterprise archive and viewer.
With these decisions locked, the essential CVIS integrations below become predictable and testable instead of fragile and ad hoc:
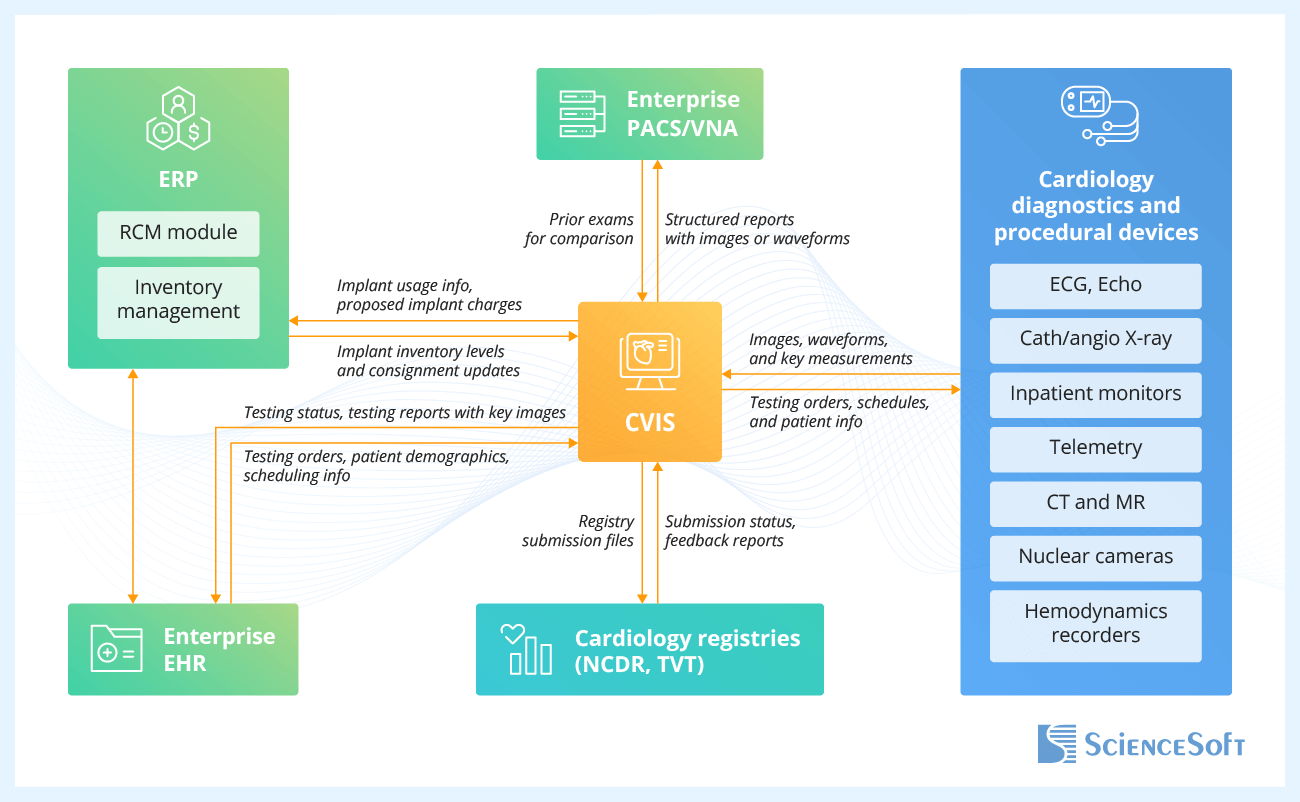
- Enterprise EHR — to anchor cardiology orders, scheduling, patient context, and testing results in one place; to spare physicians from re-entry and tab switching by allowing them to open the correct study in the CVIS viewer through single sign-on.
- Enterprise PACS and VNA — to enable enterprise-wide, zero-footprint web access to cardiology images and waveforms and their evaluation next to noncardiac studies; to unify test result storage and lifecycle, so prior exams are always available for comparison.
- Cardiology diagnostics and procedural devices — to stream synchronized images, waveforms, and measurements from diagnostic systems and patient monitors into structured reports in real time; to automatically deliver the scheduled exams and patient demographics from the order system to the imaging device.
- ERP (RCM and inventory management modules) — to feed validated implant usage, UDIs, and proposed charges from CVIS into billing workflows; to update implant inventory levels, consignment balances, and item pricing in real time.
- Cardiology registries (NCDR, TVT) — to submit registry harvest files to the registry portal and track the submission status; to import the institutional outcomes and benchmark reports for service-line quality improvement.
Field-Tested Recommendations for CVIS Development
During CVIS design, ScienceSoft recommends focusing on three key areas that often make or break real-world initiatives: structured reporting governance, predictable user experience, and compliance by design.
![]()
Structured report governance
- Structured report templates are most effective when they are governed and versioned centrally, with shared terminology and measurement lists across modalities and sites. This setup prevents label drift later and keeps downstream analytics and registry extracts consistent without manual relabeling.
- It also proves helpful when the report finalization workflow includes built-in checks for missing required fields, implausible values, and conflicting findings. In production, this typically means fewer late corrections and a higher acceptance rate on the first registry submission pass.
![]()
Predictable physician experience in the CVIS viewer
- Physician adoption usually goes more smoothly when CVIS performance expectations are made explicit and measurable rather than left at the level of “it feels slow.” Many projects benefit from defining a small set of reader-visible metrics, such as time to first image and time to open priors, and tracking them during development and rollout.
- Reader productivity also tends to improve when prior study prefetch, layout persistence, and smart loading of the most likely comparison exams are built into the design. In busy cath and echo labs, this often translates into shorter serial review sessions and less click fatigue at peak times.
![]()
Security and compliance by design
- CVIS initiatives are generally easier to defend in audits when the design phase already covers how electronic health information flows out of the system: to patient portals, to other clinicians, to registries, and to HIEs under the 21st Century Cures Act. Making these paths explicit during development reduces surprises later.
- Accounting for HIPAA Security Rule requirements during CVIS architecture design usually means less rework later. It forces early decisions on access control, audit logging, and encryption that fit actual cardiology workflows and data flows, rather than retrofitting controls onto processes after they are already defined.
How Much Does It Cost to Develop a CVIS?
In ScienceSoft’s experience, the cost of developing a CVIS typically ranges from $250,000 for focused extensions to over $3,500,000 for a full-scale platform. Project budgets largely depend on the number and complexity of device, EHR, and PACS integrations, invasive cardiology scope, and AI automation (registry data abstraction, image quantification add-ons, ECG triage, and more).
The table below outlines feature bundles and indicative costs for the most common CVIS implementation scenarios.
|
|
Standard functionality |
Advanced functionality |
|---|---|---|
|
CVIS extension pack
?
For specialty cardiac hospitals needing to fix critical CVIS gaps without replacing their existing platform. |
Cost: $250,000–$650,000 |
Cost: $650,000–$1,200,000+ |
|
Echo and ECG domain build
?
For multi-site ambulatory cardiology groups that prioritize unified echo and ECG domains and tight integration with their EHR. |
Cost: $450,000–$900,000 |
Cost: $900,000–$1,400,000+ |
|
Enterprise imaging convergence or migration
?
For IDNs that need to align cardiology imaging with enterprise VNA, universal viewer, and standardized analytics. |
Cost: $700,000–$1,400,000 |
Cost: $1,500,000–$2,400,000 |
|
Full-scale CVIS build
?
For specialty cardiac hospitals aiming to consolidate imaging, ECG, hemodynamics, and registries into a single enterprise CVIS. |
Cost: $1,400,000–$2,500,000+ |
Cost: $2,400,000–$3,500,000+ |
Why Choose ScienceSoft as Your CVIS Development Partner
- Since 2005 in healthcare software engineering and IT consulting.
- 150+ successful projects in the domain.
- Since 2013 in image analysis; since 1989 in data analytics and AI.
- Architecture and Solutions CoE with HIMSS-certified specialists to design secure and highly integrated CVIS even in legacy-heavy environments; in-house PMO to steer the project to success despite budget constraints and diverse clinician expectations.
- Proficiency in aligning healthcare software with HIPAA, GDPR, the 21st Century Cures Act, ONC Cures Final Rule, CEHRT, ONC HTI-1 Decision Support Interventions transparency rules, and FDA Clinical Decision Support guidance.
- Expertise in imaging and data exchange standards, including DICOM and DICOMweb, SCP-ECG, HL7 v2, FHIR, IHE XDS/XDS-I, C-CDA, USCDI, and SMART on FHIR; clinical coding and terminology standards, such as ICD-10-CM, CPT, SNOMED CT, and LOINC, and quality/registry formats QRDA and NCDR. HL7® FHIR® certified implementers on the team.
Certifications and awards
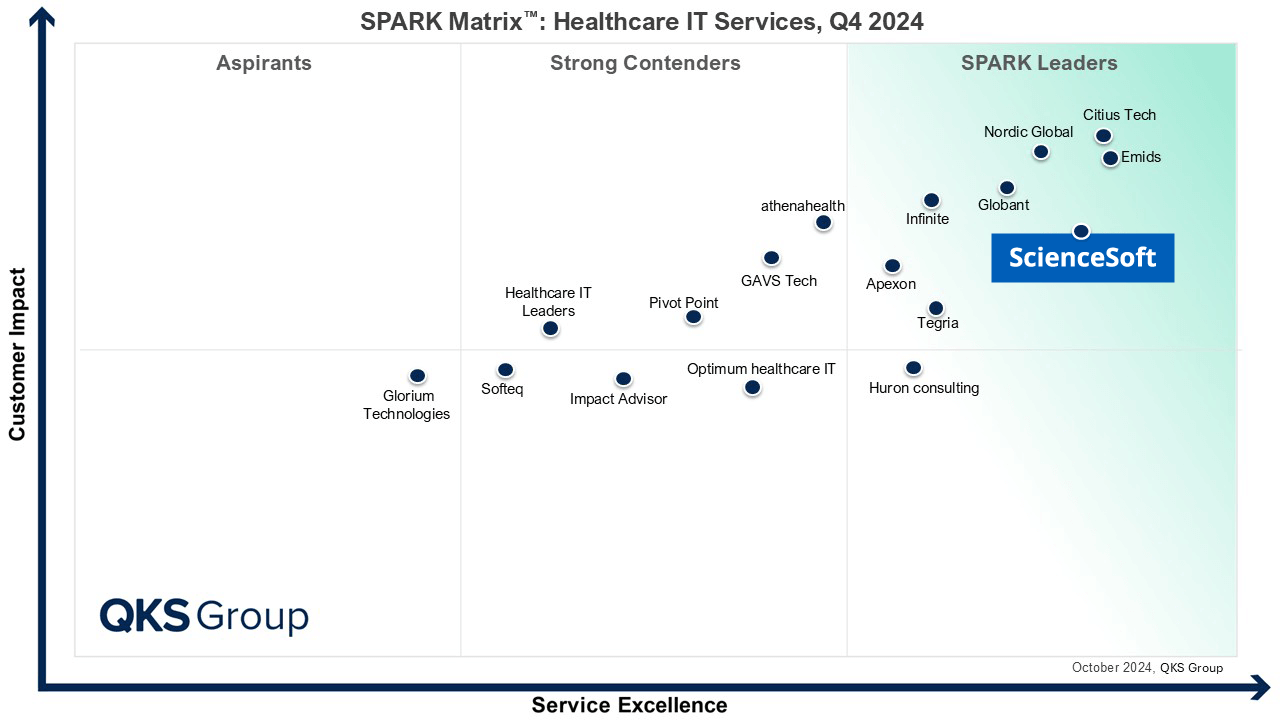
Featured among Healthcare IT Services Leaders in the 2022 and 2024 SPARK Matrix

Recognized for Healthcare Technology Leadership by Frost & Sullivan in 2023 and 2025
Named among America’s Fastest-Growing Companies by Financial Times, 5 years in a row
Top Healthcare IT Developer and Advisor by Black Book™ survey 2023

Four-time finalist across HTN Awards programs

Named to The Healthcare Technology Report’s Top 25 Healthcare Software Companies of 2025

HIMSS Gold member advancing digital healthcare

ISO 13485-certified quality management system

ISO 27001-certified security management system
What Our Healthcare Clients Say

Working with ScienceSoft was a pleasure from A to Z. Their deep knowledge of the healthcare industry specifics and DICOM standard helped us create the back end of the software for our ultrasound scanner.
We are grateful for their can-do attitude, responsiveness, and straightforward communication. RIVANNA already witnessed tangible benefits of our cooperation. We have more projects to come and are looking forward to working with ScienceSoft again.

bioAffinity Technologies hired ScienceSoft to help in the development of its automated data analysis software for the detection of lung cancer using flow cytometry. Our project required a large amount of industry-specific methodology and algorithms to be implemented into our new software connected to EHR/LIS systems, which the team handled well.
They are reliable, thorough, smart, available, extremely good communicators, and very friendly. We would recommend hiring ScienceSoft to anyone looking for a highly productive and solution-driven team.

During our cooperation, ScienceSoft proved to have vast expertise in the Healthcare and Life Science industries. They bring top-quality talents and deep knowledge of IT technologies and approaches in accordance with ISO13485 and IEC62304 standards.
I would also like to point out that ScienceSoft’s team demonstrated a great engineering culture, a proactive approach to work, and the communication was easy and clear. I would certainly recommend ScienceSoft as a reliable partner in IT consulting.
