AI for Patient Instruction Automation and Discharge
Capabilities, Architecture, Costs
With healthcare software engineering experience since 2005, ScienceSoft helps hospitals implement AI for patient instruction automation and discharge. We help hospitals create safer, faster, and auditable transition-of-care workflows that reduce avoidable friction across clinicians, nurses, case managers, patients, caregivers, and downstream care providers.

Contributors

Senior Healthcare IT & AI Consultant, ScienceSoft

Head of AI, Principal Architect, ScienceSoft
The Essence of AI for Discharge and Patient Instruction Automation
AI for discharge and patient instruction automation helps healthcare organizations speed up discharge workflows, reduce administrative burden on care teams, improve the clarity and consistency of discharge instructions, and promote safer care transitions.
When deployed in real hospital environments, such solutions typically combine several AI and automation components:
- Large and small language models (LLMs or SLMs) draft discharge summaries and instructions.
- Knowledge retrieval mechanisms (e.g., RAG or GraphRAG) ground AI outputs in approved clinical sources and patient-specific health records.
- Deterministic rule engines check medications, follow-ups, and escalation triggers.
- Traditional machine learning models may be added to estimate readmission risk, length of stay, or expected discharge date.
How AI Can Improve Discharge Outcomes
![]()
Less time spent on discharge documentation
Discharge often slows down when clinicians must manually assemble information already scattered across notes, orders, medication lists, and care plans. AI can reduce this work by preparing review-ready drafts and highlighting missing inputs before final approval.
![]()
Faster discharge readiness
Delays often come from late documentation, incomplete instructions, or unresolved follow-up details. AI helps surface these gaps earlier, so staff can correct them before the patient is ready to leave.
![]()
Fewer routine clarification calls
Many post-discharge calls happen because patients are unsure what to do, when to do it, or which symptoms require attention. AI can help make approved instructions more specific, easier to navigate, and available in patient self-service channels.
![]()
Better follow-through after discharge
Patients may miss follow-ups or home-care steps when instructions are hard to understand or aren’t reinforced after discharge. AI-supported reminders and action prompts can keep already-approved next steps visible after the patient leaves the hospital.
![]()
More consistent transition-of-care communication
Handoffs become riskier when discharge summaries, patient instructions, and follow-up plans tell slightly different stories. AI can help align these materials around the same approved source data and flag inconsistencies before they reach patients or downstream providers.
![]()
Earlier operational planning
Care coordinators and unit managers often need to know which patients are likely to leave soon and where discharge workload may build up. AI-based operational forecasting can support staffing, education, and outreach planning without making autonomous clinical decisions.
How AI for Patient Instruction Automation and Discharge Works
Common use cases
![]()
Drafting discharge summaries
Clinicians can use AI-assisted drafting inside their EHR workspaces to prepare discharge summaries faster. A language model can draft the narrative sections using relevant EHR data, while rule-based checks compare the draft against authoritative discharge sources, such as discharge orders, medication reconciliation data, prescribed discharge medications, pending tests, and follow-up plans. The clinician reviews, edits, and approves the final summary before it is saved in the EHR.
![]()
Building patient-friendly discharge instructions
AI can act as a personalization layer on top of approved discharge content. It can draft plain-language discharge instructions or after-visit summaries using available discharge information, hospital-approved templates and educational materials, medication reconciliation data, follow-up orders, and care plan details. The instructions can be adapted to the patient’s language, age, health literacy level, treatment plan, and care setting. A clinician always reviews the AI-generated instructions for completeness and safety before sharing them with the patient.
![]()
Creating post-discharge action lists and reminders
Agentic AI can extract next steps from clinician-approved discharge instructions and auto-transform them into action points executed through other systems. For example, it can identify approved follow-up items, such as appointments to book, tests to complete, or home-care steps to follow, already listed in the discharge instructions. These items can then be displayed as action points for the patient or passed to the patient notification and appointment scheduling workflows.
![]()
Answering discharge-related patient questions
AI can serve as a patient-facing assistant helping patients find and understand approved discharge information via the portal, mobile app, or an AI-supported call center. The assistant identifies the patient’s intent, retrieves relevant content from approved discharge instructions and patient education materials, and presents it in plain language following preset response templates and safety protocols. Questions that are urgent, complex, unclear, or outside the approved content scope are escalated to staff. This helps prevent AI from giving free-form medical advice or inventing discharge guidance.
![]()
Discharge planning insights
AI can support administrative and operational discharge planning by estimating likely discharge dates, expected length of stay, and follow-up workload by unit, department, or discharge pathway. These insights help care coordinators, discharge planners, and department managers plan staff time, prepare discharge education, and organize post-discharge outreach capacity.
Reference architecture
Below, ScienceSoft’s solution architects show a reference architecture for AI-powered discharge and patient instruction automation. In this setup, AI is implemented as a shared service layer that connects to the hospital’s existing EHR, patient portal, and care-management tools without replacing or altering their core functionality.
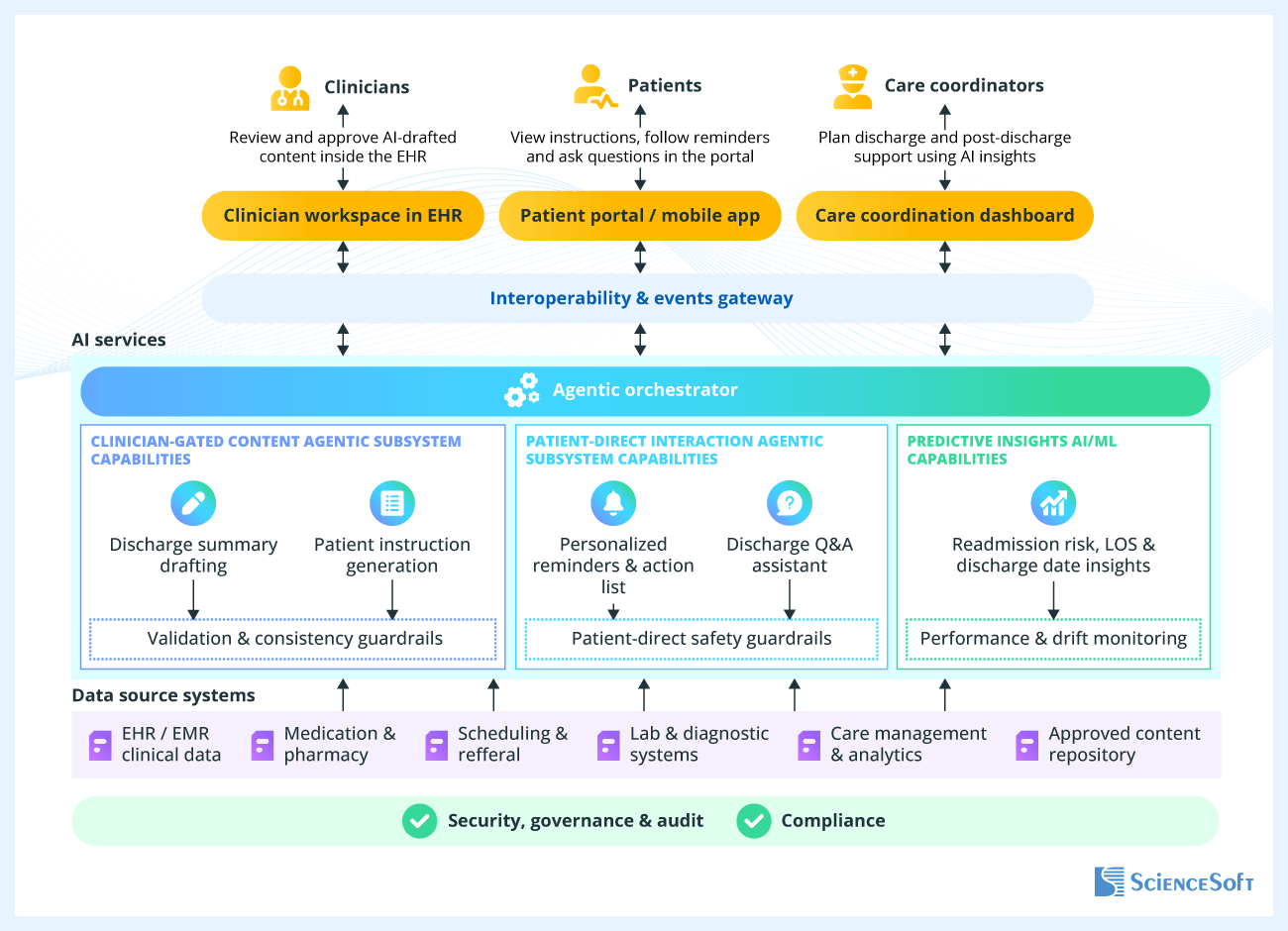
Instead of placing separate AI features inside each application, the architecture centralizes AI capabilities and makes them available through the EHR, patient portal or mobile app, and care coordination dashboard.
Clinicians interact with AI-generated content inside the EHR, where they can review, edit, and approve discharge summaries and patient instructions. Patients access approved discharge information, reminders, and Q&A support through the patient portal or mobile app (or, in more complex setups, via an AI-supported call center). Care coordinators use dashboard insights to plan discharge and post-discharge support.
The interoperability and events gateway connects these systems with the shared AI layer. It routes relevant clinical and operational data from the EHR and connected systems to AI services and returns outputs to the right destination, such as an EHR draft area, patient portal, reminder workflow, or care coordination dashboard.
The AI layer uses different automation patterns depending on the task. Generative AI (language models) drafts discharge content and plain-language instructions using approved clinical sources. Retrieval and grounding mechanisms limit patient-facing answers to approved discharge instructions, patient education materials, and permitted chart data to reduce the risk of hallucinations. Rule-based checks and deterministic validation logic can compare AI-generated content against discharge orders, medication reconciliation data, prescribed discharge medications, pending tests, and follow-up plans before clinician approval.
For discharge planning, predictive models (this is not generative AI but traditional machine learning) can also be used to analyze live and historical hospital data, including current encounter information, care plans, prior utilization, and readmission outcomes. Their outputs are returned as staff-review signals, such as readmission risk indicators, likely length of stay, and expected discharge date, rather than autonomous care prioritization decisions.
Security, compliance, and governance controls are built into the architecture wherever PHI is accessed, processed, or returned to users. They include role-based access, authenticated EHR and portal integrations, encryption in transit and at rest, PHI redaction where appropriate, and audit logging of key AI-related actions, such as generated outputs, model or prompt versions, clinician edits, approvals, and patient-facing releases. These controls help to keep AI-supported discharge workflows traceable, reviewable, and aligned with internal safety and compliance requirements.
From my experience, a frequent mistake in integrating AI into charting and discharge workflows is treating the AI draft as a separate recommendation window that sits beside the chart. This only adds work for clinicians and requires extra attention span, so it usually gets ignored. A much better approach is to have the AI output land directly in the clinician's draft area in the EHR, so they can review and approve it as their own work. This is really the only way to save time in practice.
Also, from day one, track how much clinicians edit AI-generated drafts before approving. If edits are rare and local, your AI is doing a good job. But if edits are frequent or clinicians rewrite entire sections, you may have a hallucination or data retrieval problem, not an adoption problem. You’re not saving much of clinicians' time if their real workload has simply shifted from writing to editing.
Key Challenges of Implementing AI for Patient Instruction Automation and Discharge
Challenge #1: AI may generate incorrect or incomplete summaries, patient instructions, or answers to patients’ discharge-related questions.
Solution:
ScienceSoft designs AI-assisted discharge workflows so that the AI drafts summaries and patient instructions using only defined inputs: the EHR data, medication reconciliation results, prescribed discharge medications, follow-up orders, pending tests, care plan, hospital-approved templates, and patient education materials.
However, even when using only data from approved sources, an AI-generated instruction can still be unsafe or incomplete. For example, it may omit an ordered follow-up test or repeat an outdated medication dose. To catch these issues, we add hard validation rules to compare the draft with source data and flag missing, conflicting, or unsupported items for correction before clinician review.
Clinicians remain responsible for approving discharge summaries and patient instructions before they are saved in the EHR or shared with patients. For patient-facing Q&A, the assistant answers only from approved instructions, education materials, and permitted chart data. Questions about new symptoms, medication changes, worsening condition, emergencies, or anything outside the approved discharge plan are routed to staff. This helps hospitals use AI to speed up discharge communication without turning it into unsupervised medical advice.
Challenge #2: AI-powered discharge workflows may involve multiple vendors and processing environments, making it difficult for hospitals to control where PHI is processed, stored, retained, and used.
Solution:
ScienceSoft starts by defining where PHI is allowed to go before selecting AI services or designing integrations. For some hospitals, this means using a HIPAA-eligible cloud service and BAA-covered AI provider. For others, it means keeping AI processing inside the hospital’s own cloud or on-premises environment when external processing is not acceptable.
With AI involved in medical documentation, PHI can move through more places than you initially expect: the EHR, integration layer, AI service, logs, monitoring tools, backups, support workflows, and patient-facing channels. If these paths are not mapped early, a hospital may later discover that discharge data is retained by a vendor, processed in a foreign region, stored in logs, or used in other ways its compliance team has not approved.
To prevent this, we map PHI flows across all systems and vendors, then configure least-privilege access, encryption, authenticated EHR and portal integrations, PHI access logging, and audit trails for AI-related actions. We also help verify vendor-side terms, including BAA coverage, retention rules, processing location, no-training commitments, and the split of responsibilities between the hospital, ScienceSoft, the cloud provider, and the AI service provider.
Technologies We Use to Implement AI for Discharge and Patient Instruction Automation
AI implementation and model development
Foundation LLMs and AI services
- Azure OpenAI Service
- Amazon Bedrock
- Llama
- Mistral
- MedLlama
AI application layer
- Python
- FastAPI
RAG, search, and grounding
- Pgvector
- Azure AI Search
AI guardrails and PHI protection
- NVIDIA NeMo
- Microsoft Presidio
- Azure AI Content Safety
Predictive modeling
- XGBoost
- LightGBM
Feature store, MLOps, and AI observability
- Databricks
- Feast
- Databricks MLflow
- Langfuse
- Evidently AI
Software engineering, integration, and deployment
Cloud and healthcare data platforms
- Microsoft Azure
- Amazon Web Services
- Google Cloud Platform
- Azure Health Data Services
- Amazon HealthLake
- HAPI FHIR
Web and mobile technologies
- React JS
- Next.js
- React Native
Data, messaging, and event streaming
- PostgreSQL
- Apache Kafka
- Azure Event Hubs
Containers, orchestration, and GitOps
- Docker
- Kubernetes
- HashiCorp Terraform
- Argo CD
- GitHub Actions
Identity, access, security, and monitoring
- Microsoft Entra ID
- Okta
- HashiCorp Vault
- Splunk
- Microsoft Sentinel
Patient communication
- Twilio
Analytics and dashboards
- Power BI
- Innovaccer
Costs of Implementing AI for Discharge and Patient Instruction Automation
The cost of implementing AI for discharge and patient instruction automation typically ranges from $100,000 to $1,000,000+ and depends mainly on the scope of AI-assisted discharge workflows, integration complexity, patient-facing functionality, validation needs, and governance requirements.
At the lower end of this range, hospitals may implement a narrow AI module, such as AI-assisted discharge summary drafting or patient instruction generation within an existing EHR workflow. At the higher end, the scope may expand to a broader shared AI layer that additionally supports patient portal or mobile delivery, reminders, Q&A, predictive discharge planning insights, and multiple hospital system integrations.
Key cost drivers for implementation include:
- The number and complexity of AI use cases that must be covered.
- The number and complexity of integrations.
- The quality, structure, and accessibility of clinical and historical data, especially if predictive models (e.g., for readmission risk or expected discharge date) are included.
- Auditability, security, and compliance requirements for patient-facing and clinician-facing outputs.
- The number of patient-facing channels covered (e.g., portal, mobile app, SMS, or email).
- The need for new patient-facing or care-team interfaces, for example, a discharge dashboard or a portal assistant.
- The chosen deployment model and operating setup.
Why ScienceSoft
- In healthcare IT since 2005.
- In AI since 1989, with experience in building custom AI models and adapting pretrained ones.
- 150+ successful healthcare IT projects.
- 750+ experts, including AI engineers, MD consultants, software developers, integration specialists, security experts, and QA engineers.
- Deep knowledge of healthcare interoperability and EHR integration standards, including HL7 v2 and v3, FHIR, SMART on FHIR, and C-CDA.
- Experience supporting compliance with HIPAA/HITECH, GDPR, Saudi PDPL, and more.
- An in-house PMO to keep complex healthcare IT projects predictable, transparent, and aligned with the planned scope, timelines, and risk controls.
- Architecture & Solutions Center of Excellence to design secure, scalable, and integration-ready architectures for hospital AI initiatives.
- Strong security and quality management practices backed by ISO 27001 and ISO 9001 certifications.
Certifications and awards
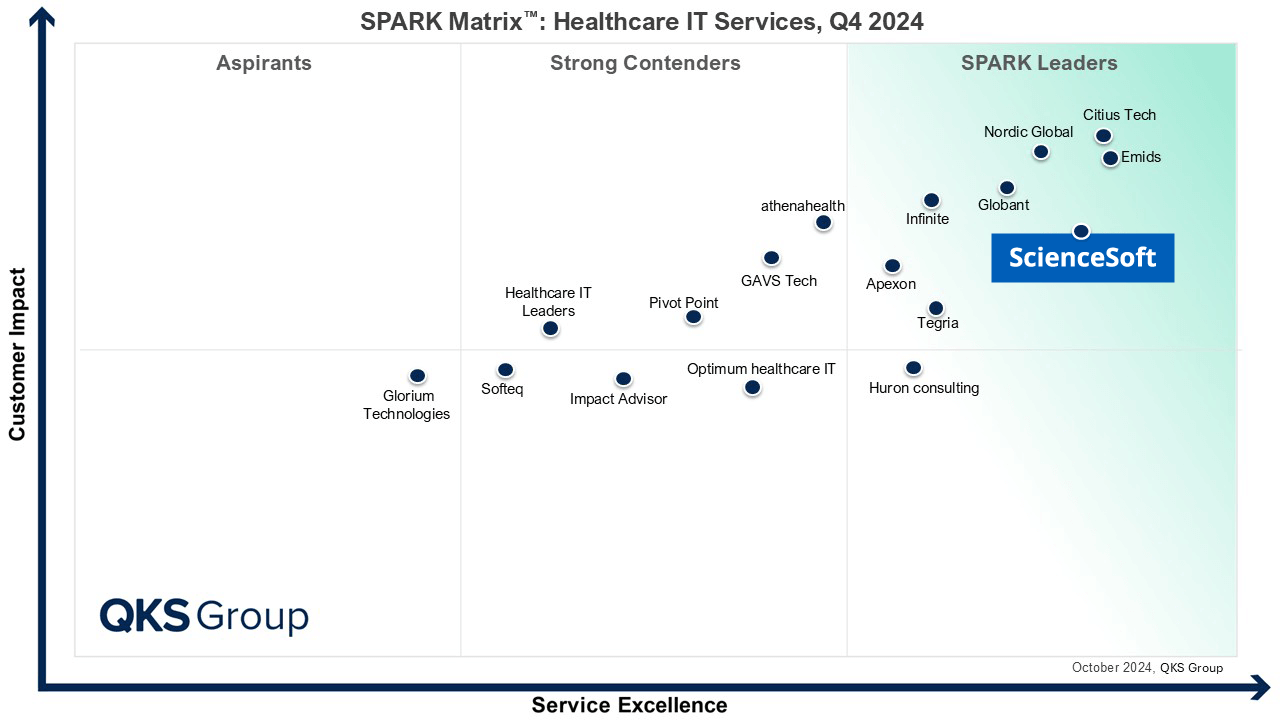
Featured among Healthcare IT Services Leaders in the 2022 and 2024 SPARK Matrix

Microsoft Solutions Partner for Data & AI
Named among America’s Fastest-Growing Companies by Financial Times, 5 years in a row

Recognized for Healthcare Technology Leadership by Frost & Sullivan in 2023 and 2025

Four-time finalist across HTN Awards programs
Top Healthcare IT Developer and Advisor by Black Book™ survey 2023

HIMSS Gold member advancing digital healthcare

ISO 13485-certified quality management system

ISO 27001-certified security management system
What Our Clients Say

Our project required a large amount of industry-specific methodology and algorithms to be implemented into our new software connected to EHR/LIS systems, which the team handled well. <…> They are reliable, thorough, smart, available, extremely good communicators, and very friendly.

They delivered a fully customized AI medical chatbot PoC in just two weeks, which was unbelievable. <...> I’m genuinely grateful to ScienceSoft for their hard work and would absolutely recommend them to anyone looking for top-notch results in health tech.

The resulting Proof of Concept exceeded expectations, and we sincerely appreciated the way it was delivered. We found ScienceSoft to be dependable and forward-thinking, and we would confidently recommend them for high-responsibility projects.


