Utilization Management Software for Healthcare Providers
Core Workflows, Integration Map, Costs
In healthcare IT since 2005, ScienceSoft designs utilization management solutions for provider organizations that help clinical and administrative UM teams reduce manual tracking and speed up payer follow-ups through a single case workflow.

Contributors

Senior Healthcare IT & AI Consultant, ScienceSoft

Head of AI, Principal Architect, ScienceSoft
Utilization Management Software Explained
Utilization management (UM) software is a clinical-and-coverage workflow system used by healthcare workers to manage insurer authorizations in a consistent, time-bound, and trackable way. Utilization management solutions turn a patient episode into a set of guided steps: confirm the insurer and plan, route the case to the appropriate reviewer, pull key details from the EHR, and document level-of-care and continued-stay reviews with supporting notes and results.
Demand for dedicated UM software is growing, especially since prior authorization remains a major UM bottleneck for many providers. According to AMA, 93% of physicians report that prior authorization delays access to necessary care, and practices report that physicians and staff spend an average of 13 hours per week on prior authorization work. This friction also affects workforce sustainability, with 89% of physicians saying prior authorization somewhat or significantly increases burnout.
To relieve these pressures at the most delay-prone point of the UM workflow — and to prevent downstream rework across related UM steps — providers implement custom utilization management solutions as data integration layers, custom EHR modules, or even full-scale systems. Some providers also choose to modernize their existing UM tools due to the limitations of out-of-the-box software. These custom solutions reduce turnaround time and target delays across the UM chain by:
- Centralizing the case record so insurance details, request status, clinical evidence links, and submission history live in one place, rather than being re-entered across tools.
- Automating data capture and checks by prefilling key fields from existing systems.
- Cutting rework from incomplete submissions by prompting for missing documents before the case is submitted.
- Making deadlines and workload visible with due dates and at-risk indicators that help teams prioritize and avoid late actions.
Custom UM software implementation cost varies between $200,000+ for an EHR extension to $1,000,000+ for a full-scale system. Use our free online calculator to get a cost estimate for your case.
Utilization Management vs. Utilization Review
You may often hear “UM” and “UR” used interchangeably. However, utilization management (UM) is a broader workflow that usually includes case routing and review, documentation exchange, status tracking, and appeals — basically, the entire chain of payer communication. Utilization review (UR) is just a step in that workflow, where medical necessity and level of care are documented.
Core Capabilities of Utilization Management Software
Below is a practical set of capabilities that healthcare organizations often request when implementing a UM solution. We shape each implementation around the existing UM process, insurer requirements, and integration landscape, so the final workflow steps and modules may vary by organization.
![]()
Case intake
Case records can be created from various entry points, such as an EHR trigger, a portal submission, a fax-to-PDF upload, or phone intake. Plan and member details can be automatically pulled from registration data or entered manually. Based on the insurer and request type, the case surfaces required fields, documents, and due dates. The system flags missing or conflicting insurance information early and routes the case into follow-up instead of letting incomplete requests move into review.
![]()
Case routing
New cases are placed into the correct work queue based on request type, urgency, site, and insurer rules. Worklists can highlight priority, due dates, and follow-ups so teams see what is currently at risk. Status changes follow the rules you can set, so case progress is both consistent and traceable (e.g., intake → in review → submitted → determination received). Routing and reassignment will support workload balancing and help teams avoid unattended cases when volumes spike.
![]()
Utilization review
UR staff can complete level-of-care and medical-necessity reviews in a dedicated workspace, documenting “met/not met” findings and rationale for inpatient, post-acute, and home care decisions. To support consistent review, the workspace can show embedded criteria and the relevant chart context needed to justify the decision. Reviewers can access key evidence (e.g., recent notes, labs, imaging results) without leaving the case. The same workspace can support both initial reviews and scheduled continued-stay reviews, all tied to the case history.
![]()
Escalation and collaboration
When a case is borderline or requires a higher-level decision, UM nurses can route it to a physician advisor worklist with a clinical summary and direct links to supporting chart context. Secure case comments and tasks, as well as collaboration items (requests for clarification, documentation needs, peer-to-peer coordination), will be kept in a single case thread with time stamps for convenience.
![]()
Prior authorization
A document packet builder streamlines assembly of insurer-ready submissions for prior authorization. Insurers can receive packets through any supported channel (portal, clearinghouse EDI, or FHIR prior-authorization endpoints). Packet history allows resubmissions if more information is requested, so the case can be updated and not rebuilt from scratch. Continued-stay work can be scheduled as follow-up reviews, with due dates and PA details.
![]()
Appeals
Case history can help with appeal creation and tracking. Staff can reuse the existing evidence set and add any missing support from the chart. Deadlines, appeal levels, and outcomes are tracked on the same timeline as the original request so teams can see what triggered the appeal and what changed. Letter templates can be added to reduce manual rewriting and keep rationale consistent when drafting appeal documentation.
![]()
Reporting and retrospective insights
UM leaders can track processing time, denial reasons, approval rates, and appeal overturns in real time. Dashboards can break trends down by payer, service line, facility, request type, and reviewer to show where delays and denials concentrate. The same reporting layer can support retrospective review by highlighting post-service denials and repeat documentation gaps, so teams can target audits, education, and process fixes.
AI Capabilities for Utilization Management
![]()
AI for intake cleanup and completeness
An AI copilot can help UM coordinators turn messy submissions into usable cases: extract key fields from attachments (e.g., referral notes, imaging reports, discharge summaries), detect missing items, and generate a “missing info” checklist before a nurse even touches the case.
![]()
AI for chart summarization and evidence packaging
AI assistants can support reviewers by summarizing the relevant clinical story (incl. timeline, severity indicators, failed conservative therapy, functional status) and producing a structured clinical summary that is easier to review and attach to an insurer submission.
![]()
AI for UM decision support
AI can recommend next-best actions using internal procedures and rulebooks: it can suggest which medical policy to apply, what documentation supports it, and whether the request appears to meet the criteria. All AI reasoning remains traceable and auditable because it is tied to specific entries in the internal knowledge base.
I’d like to address the likely skepticism here: I know many clinicians are cautious about AI in utilization work. This is a viable concern, and for a hospital utilization management solution, the safest approach is to introduce AI as a helper, not a decision-maker. Let it pull key details from the chart, summarize the case, and flag missing documents before physician advisor review and before prior authorization submission to the payer. It can even suggest the most likely next step, like which form to use and what information still needs to be added. But all of these functions still require human sign-off, which means you will keep clinical judgment and final sign-off with people. This will speed up paperwork without replacing clinical review or making risky decisions.
Important Integrations for a Utilization Management System
To automate clinical utilization work end to end, a UM solution typically needs to connect to other healthcare systems that hold the needed data and trigger the next steps. Below are the key systems that usually provide relevant information and updates. Your integration map may differ, depending on your IT setup and which parts of the workflow you want to automate.

- EHR (clinical + registration) brings verified plan details and clinical evidence into the UM workspace, so nurses and physician advisors don’t have to retype data or chase notes.
- Payer connectivity solutions support sending prior authorization and utilization review requests and receiving decisions across common payer routes. This can include multi-payer portal networks, payer-specific portals, electronic transactions through a clearinghouse (X12 278 with X12 275 attachments), and FHIR-based prior authorization where supported.
- Document imaging / ECM supplies the documents that are not created in the EHR, such as faxed notes, referral forms, signed orders, and payer letters. The UM system can pull these files into a case, attach them to a submission packet, and keep a reference to the original stored document for audit.
- Patient accounting and billing / RCM systems use authorization details during claim preparation and denial prevention, and it is also the source of claim outcomes that can feed UM follow-ups and appeals.
Development Tips for Implementing Utilization Management Solutions
![]()
Build packet handling instead of basic uploads to reduce rework and delays
Instead of storing attachments as a list, it’s more useful to design a document packet workflow inside each authorization request. Create a packet entity with required document types (e.g., clinical notes, imaging, lab results), a checklist mapped to payer requirements, and versioned packet submissions (e.g., Draft - Submitted - Returned). Add rules that mark items as missing until the right document type is attached, prevent submission when required items are incomplete, highlight the latest packet version, and log who added or changed each file and when. This turns uploads into a controlled submission process, reducing back-and-forth and avoidable denials caused by incomplete packets. Expose this as a “Packet tab” on the request page with a checklist view, a version history panel, and a “Submit packet” action that locks the version and generates the payer submission package.
![]()
Make physician advisor reviews easy to minimize adoption risks
Physician advisors live in the EHR, so an efficient utilization management tool must minimize context switching. We suggest building an EHR-first review experience: surface UM review requests in the EHR (as an embedded view or a deep link to the exact chart section) and keep the UM page as a fast fallback. Each review request should open with a concise clinical summary, the reason for escalation, and the supporting chart link. Provide one-click response actions for the most common outcomes (approve, deny, request more info, schedule peer-to-peer) so advisors don’t default to phone calls and side messages. Track advisor response time per case for UM operations and medical management to monitor turnaround and bottlenecks.
![]()
Show deadlines in daily work to prevent overdue and late actions
Since UM work is time-bound, a common usability issue might appear when deadlines are buried in a detail view or visible only to managers, so frontline staff do not see what is due until it is late. Deadline visibility needs to be built into the daily flow: due dates and “at risk” cues should appear in UM work lists and case headers, and there should be reminders and manager views for overdue items. This makes prioritization obvious, reduces rushed decisions, and helps teams stay inside payer timeframes.
Healthcare Utilization Management Solution Costs
Custom utilization management (UM) software solution costs typically range from $200,000 to $1,000,000+.
![]()
$200,000–$600,000+
We add a focused UM layer to an existing EHR for provider organizations. It usually includes core UM modules and data views. This is generally a good option when you want to improve UM work routines without deploying a separate utilization management application.
![]()
$300,000–$700,000+
We extend an out-of-the-box UM product already in use. Typical choice when the UM tool is already deeply embedded in the provider’s operations, but it creates delays, rework, or poor visibility due to the lack of functionality or integrations.
![]()
$600,000–$1,000,000+
We deliver a full-scale provider UM platform integrated with upstream and downstream systems, including EHR and payers’ endpoints. Best option for a large provider looking to implement UM as a strategic system across multiple sites and service lines and requiring enterprise-grade governance, auditability, and rollout control.
Want a more precise figure?
ScienceSoft's team is ready to provide a quote for your specific case.
Our Clients Say
Todd Nilson
MD
We are thankful for the meticulous and value-driven approach of ScienceSoft’s team. They created comprehensive project documentation, feature lists, and worked out thorough recommendations to help us improve the stability and performance of our solution.

Working with ScienceSoft was nothing but a learning experience <…>. They’re very responsive and very knowledgeable. I recommend ScienceSoft for any needs and will work with the company again if needed in the future!

ScienceSoft has been a competent partner for medical software development. We would recommend them as a trustworthy vendor. They are reliable, thorough, smart, available, extremely good communicators and very friendly.

They collaborated with our medical professionals with great professionalism and care <…>. We found ScienceSoft to be dependable and forward-thinking, and we would confidently recommend them for high-responsibility projects.

With ScienceSoft on our side, we can fully focus on delivering tailored healthcare solutions to our clients. Highly recommend them!


Why Implement a Utilization Management Solution With ScienceSoft
-
Since 2005 in healthcare software engineering and IT consulting.
- 150+ successful projects for healthcare organizations and healthtech vendors.
- Architecture and Solutions CoE to design UM solutions that are secure, integrated, and easy to govern at scale over time.
- In-house compliance officers to design UM solutions with HIPAA-aligned safeguards that support audit-ready utilization review documentation.
- Expertise in interoperability standards, including FHIR and HL7 v2/v3.
- Experience with payer prior authorization transactions (X12 278) and related attachment processing (X12 275), as well as CAQH CORE operating rules.
Certifications and awards
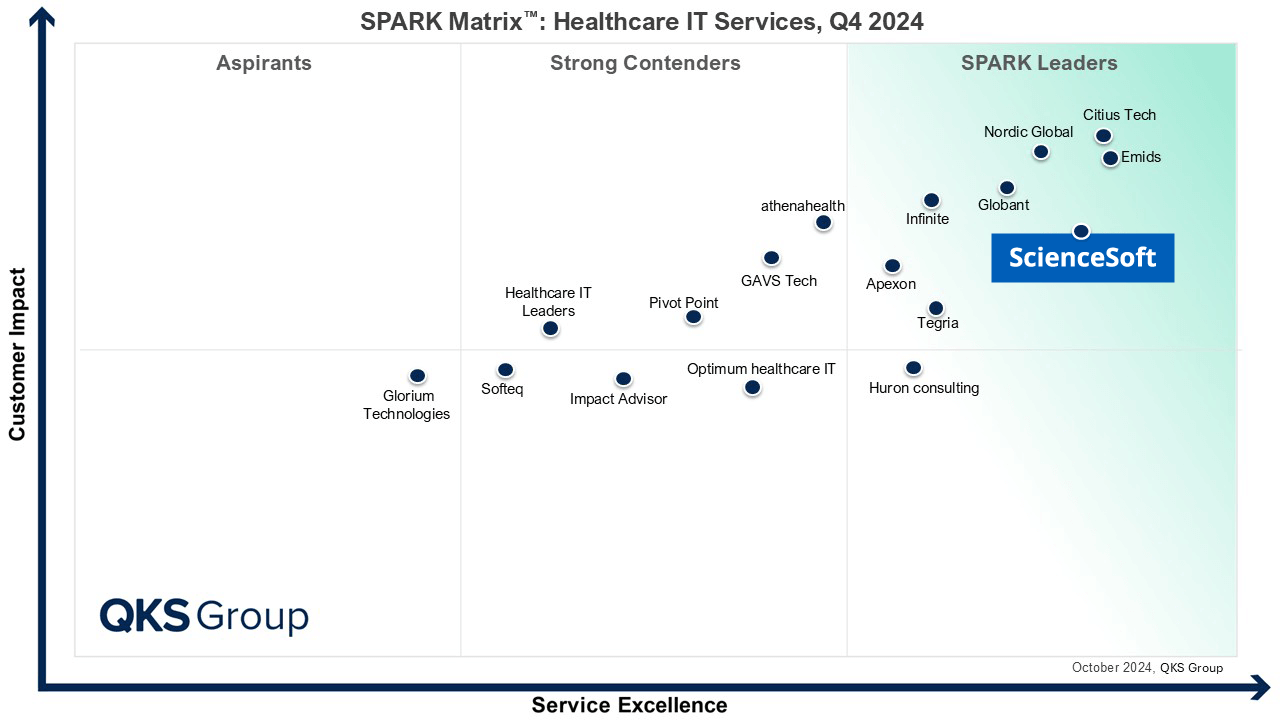
Featured among Healthcare IT Services Leaders in the 2022 and 2024 SPARK Matrix

Recognized for Healthcare Technology Leadership by Frost & Sullivan in 2023 and 2025
Named among America’s Fastest-Growing Companies by Financial Times, 5 years in a row

Four-time finalist across HTN Awards programs

Named among Becker’s Telehealth Companies to Know in 2026

Named Leading Healthcare Software Provider 2026 at Global Health & Pharma’s Healthcare & Pharmaceutical Awards

HIMSS Gold member advancing digital healthcare

ISO 13485-certified quality management system

ISO 27001-certified security management system
