AI for Patient Records Management
Architecture, Functionality, and Costs
In AI since 1989 and in healthcare IT since 2005, ScienceSoft designs secure and compliant AI solutions for medical providers and healthcare software product companies.

AI-Driven Patient Records Management in a Nutshell
Artificial intelligence (AI) solutions for patient record management leverage natural language processing, predictive text, intelligent search, and other techniques to optimize administrative workflows. AI algorithms can streamline clinical documentation by automating patient data entry, categorization, and retrieval, allowing clinicians to focus on patient care.
Medical AI Market Overview
The global healthcare AI market was valued at $20.9 billion in 2024 and is estimated to reach $148.4 billion by 2029, registering a CAGR of 48.1% during the forecast period. The key market drivers include the generation of large and complex healthcare datasets, the pressing need to reduce healthcare costs, and the shortage of healthcare workers. 56% of physicians consider administrative workflow automation the best way to leverage AI technology.
How AI Can Support Patient Records Management
![]()
Large language models (LLMs) can transcribe patient-doctor conversations or clinician dictation and extract key clinical facts such as symptoms, diagnoses, medications, allergies, and procedures. These elements can then be normalized to standard terminologies and mapped into structured record fields to maintain consistency. All AI-generated content remains editable and subject to clinician approval before it is committed to the official medical record.
![]()
External record integration & reconciliation
LLMs can review incoming referrals, discharge summaries, and other outside records, identify clinically relevant facts and key new findings. Then they compare these elements with the existing chart to identify duplicates, outdated entries, or conflicting information. When differences are detected, AI can summarize them and suggest updates for review. This approach helps integrate outside information while preserving longitudinal data integrity and traceability. Similar AI capabilities are increasingly used for AI-assisted medication reconciliation and drug interaction review, where medication information from multiple sources must be consolidated and validated.
![]()
Record search & summarization
Instead of scanning dozens of notes, staff can request focused views such as recent cardiac history, medication changes over time, or diagnostic events tied to a particular condition.
Graph-based retrieval techniques (GraphRAG) can help LLMs identify relevant chart elements by following relationships between events and clinical concepts, improving coverage compared to keyword or similarity search alone. The system then organizes results chronologically and links them back to the source documents for validation.
![]()
Prior authorization documentation support
AI can assist administrative staff with prior authorization documentation by locating supporting evidence across the chart and organizing it in accordance with payer requirements. Relevant diagnoses, prior treatments, test results, and clinical rationale can be extracted from notes and structured fields and compiled into draft requests or medical necessity letters. Rules-based logic can then compare the available documentation against payer criteria and highlight gaps before submission.
![]()
AI can support coding and billing workflows by reviewing encounter documentation for coding-relevant details and potential inconsistencies. Large language models can highlight where documentation may not fully support a proposed code and explain what’s missing in plain language. Predictive models can also identify encounters with characteristics similar to past denials or undercoding patterns, so teams can review and correct them before claims are submitted.
![]()
Registry & quality reporting automation
AI can reduce manual chart review for registry and quality reporting. Machine learning models and rules-based logic can evaluate eligibility criteria against structured data, while LLMs extract supporting evidence from clinical notes and other unstructured documents. Extracted data elements can populate reporting templates and help identify documentation gaps that may affect quality measure requirements. Where required, datasets can be de-identified before submission to registries or use in research and secondary analysis.
Get Your AI-Powered Solution
ScienceSoft is ready to develop an advanced AI-driven system for patient records management that will help clinicians reduce administrative burden.
How AI for Patient Records Works
ScienceSoft’s architects have prepared a reference architecture that illustrates how AI can be integrated into electronic health records. This architecture view focuses on how documentation is created, reviewed, finalized, and reused across coding, reporting, and analytics workflows. While the example is based on Microsoft cloud technologies, the same design can be adapted to other platforms and tools, and altered depending on the scope of automation and required functions.
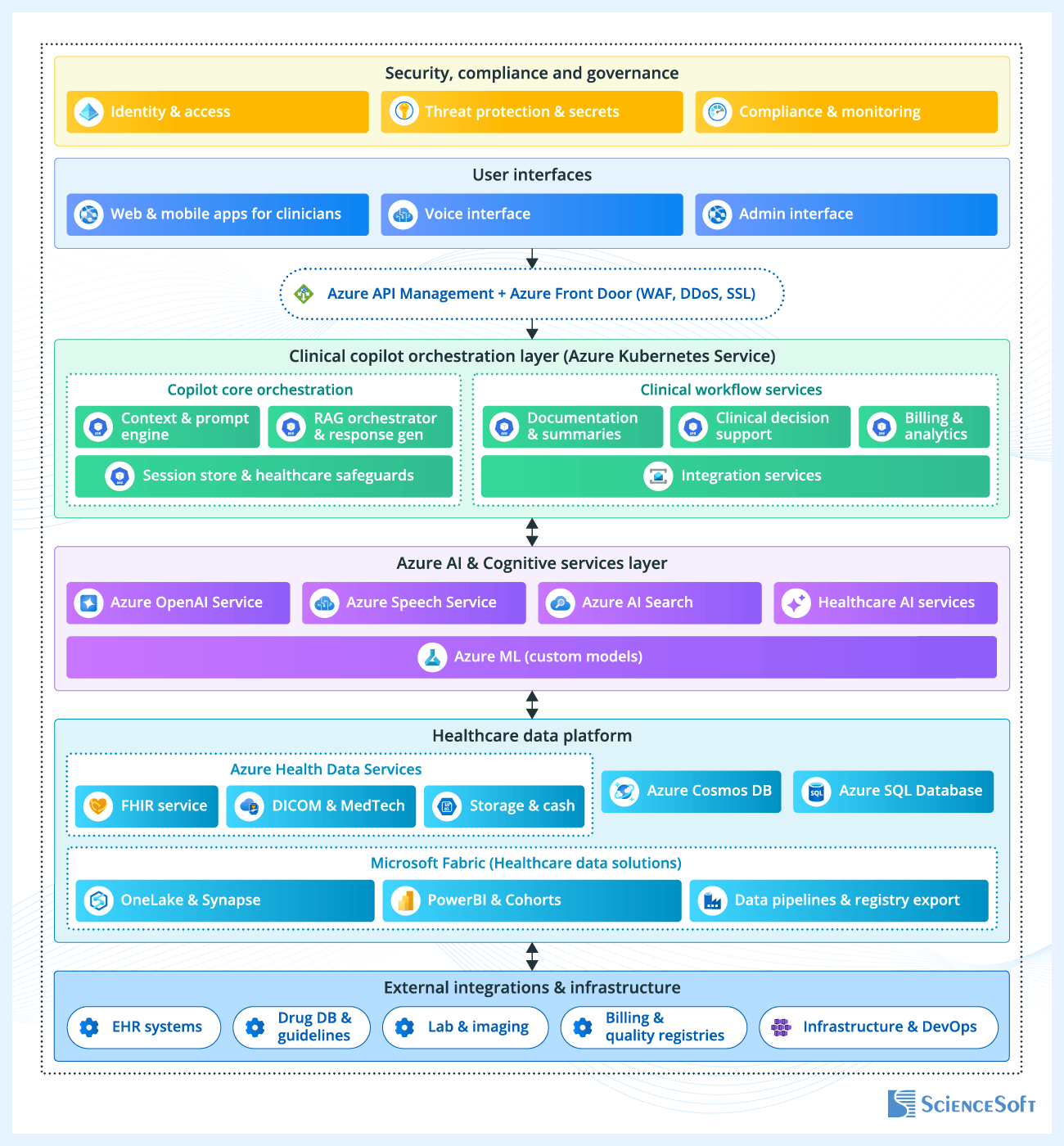
Instead of relying on a single AI component, the system distributes responsibilities across multiple services in accordance with the records lifecycle. For example, there are separate services for documentation drafting and summarization, clinical decision support, and billing and analytics. This helps providers apply individual rules and controls to AI models that access health records and adjust their capabilities without reworking the entire system.
For better accuracy, AI modules use data from existing records to ground their outputs. The system first determines which patient, encounter, and document state the current task belongs to, and then pulls in the relevant supporting data from integrated systems and data repositories. This may include unstructured notes, structured patient data, relevant clinical guidelines, and other evidence needed to complete or validate the record. AI-generated content is always tied back to these sources, so users can review where specific elements come from and identify missing or inconsistent information.
The platform also separates data storage based on how information is used. Clinical records remain in FHIR-based services for structured, standardized access to patient data. Source documents (e.g., clinical notes, transcripts, and scanned files) are stored separately as unstructured data. This allows the system to handle large, text-heavy content efficiently and retrieve it when needed for summarization or review. Finally, the data generated during AI-assisted workflows, such as session state, intermediate outputs, and interaction history, is handled in low-latency databases. This ensures that the system can respond quickly during interaction-heavy tasks such as conversational assistance, quick follow-up queries, or switching between workflow steps, without delays caused by heavier clinical data stores.
AI assists with documentation but never takes on clinical responsibilities. Drafts, suggestions, and identified gaps always go through human review before becoming part of the official record. The system enforces validation steps and requires explicit approval for any updates that affect finalized documentation or downstream processes.
Controls for security, access, and auditability extend across all stages of the records’ lifecycle. The system limits who can access or modify records, encrypts data in transit and at rest, and logs how documentation is created, updated, and used. This enables end-to-end tracing of changes and compliance with regulatory requirements such as HIPAA and HITRUST.
AI Implementation for Records Management: Success Story
|
|
Atrium Health, North Carolina’s 70,000-employee hospital network, adopted Microsoft’s DAX™ Copilot to streamline administrative processes across the organization. The solution enables the automated creation of draft clinical summaries from in-person exams or telehealth patient conversations that can be immediately reviewed and finalized in the EHR system. As a result, clinicians save up to 40 minutes per day, and 84% of them report an improved documentation experience. |

What Makes AI Scribes Worth Adopting
Hadeel Abu Baker examines why AI scribes are gaining traction in care delivery, and what can slow adoption in real settings. The interview highlights governance, human review workflows, speech accuracy, and the limits of automation.
Technologies ScienceSoft Uses to Build AI for Patient Records Management
Generative AI
Models
- Large Language Models (LLMs)
- Small Language Models (SLMs)
- Multimodal models
- Computer vision models
- Image generation models
- ASR speech models
- TTS speech models
- Speech-to-Speech Models
- Audio models
- Realtime
Model adaptation and efficiency
- Training from scratch
- Data design
- Data labelling/annotation
- Fine-tuning
- Instruction tuning
- LoRA adapters
AI platforms and services
- Azure OpenAI Service
- Microsoft Foundry
- Amazon Bedrock
- Google Vertex AI
- Google AI Studio
- Hugging Face Inference
- Oracle Cloud
- G42/Core42
- NVIDIA AI Enterprise
Agents and orchestration
- RAG
- Graph RAG
- Agentic workflows
- OpenAI Agents SDK
- OpenAI Agents (platform/guides)
- AWS Agents
- Claude Agent SDK
- Google Agent Development Kit (ADK)
- Microsoft 365 Agents SDK (Copilot Studio)
- OpenClaw
- LangChain
- LangGraph
- smolagents
- LiveKit
- Dify
- n8n
- Faiss
- ChromaDB
- Qdrant
- Weaviate
- OpenSearch
- Pgvector
- Amazon Neptune
- Graph RAG Toolkit
- Neo4j
Traditional ML
Platforms and services
- Azure Cognitive Services
- Azure Machine Learning
- Microsoft Bot Framework
- Amazon SageMaker AI
- Amazon Transcribe
- Amazon Lex
- Amazon Polly
- Google Cloud AI Platform
- Google Vertex AI
Frameworks and libraries
- Apache Mahout
- Apache MXNet
- Caffe
- TensorFlow
- Keras
- Torch
- OpenCV
- Apache Spark MLlib
- Theano
- Scikit Learn
- Gensim
- SpaCy
Healthcare-specific language models
- MedGemma
- MedLM
- BioMedLM
Speech recognition, diarization, and speech-to-speech models
- Parakeet
- Canary
- pyannote.audio
- TitaNet
- ECAPA-TDNN
- Amazon Transcribe Medical
- Google Cloud Speech-to-Text
- Amazon Nova 2 Sonic
Preventing Common Pitfalls of AI for Records Management
![]()
Handling PHI securely in AI-driven workflows
AI systems introduce additional layers of data handling (prompts, retrieved context, and intermediate outputs) that can expose more PHI than intended if left uncontrolled. Without clear boundaries, the system may retrieve broader patient data than required for a given task or include unnecessary details in generated outputs.
Solution
![]()
Making LLMs accurate and context-aware in clinical workflows
Even strong models may miss relevant clinical context, return incomplete results, or produce outputs that are correct in isolation but inconsistent, poorly structured, or not aligned with the expected clinical format.
Solution

Humans in the loop are essential for medical AI effectiveness
During the development stage, medical coders should review AI-generated documentation and edit the output when necessary. For example, if an AI-powered transcriber misinterprets a drug name, the clinician corrects it. The model can then learn from the corrections to improve its accuracy. The human-in-the-loop (HITL) approach not only helps ensure AI’s reliability but also builds care providers’ trust in the new solution as they learn to work with it.
Costs of AI-Driven Records Management Solutions
Key cost factors to consider:
- The scope of AI functionality.
- Algorithm complexity.
- The number of data sources and the volume of data for processing.
- The number and complexity of integrations with other solutions (e.g., patient portals).
- Performance, usability, security, and compliance requirements.
The costs of custom AI-enabled software for patient records management may vary from $30,000 to $800,000+. Below are sample cost ranges for commonly requested solutions.
![]()
$30,000–$70,000
For a standalone AI module that enables a single data management process (e.g., summarizing patient history or scanning handwritten text).
![]()
$150,000–$300,000
For an AI virtual assistant that can transcribe patient-doctor conversations and suggest fixes for potential errors in the physician’s input.
![]()
$400,000–800,000+
For a custom AI-powered EHR system with features like dictation, virtual assistance, and smart billing (enables AI-driven insurance eligibility checks and in-line suggestions of billing codes).
Insights From ScienceSoft's Healthcare IT Experts

Hadeel Abu Baker
Senior Healthcare IT & AI Consultant, ScienceSoft
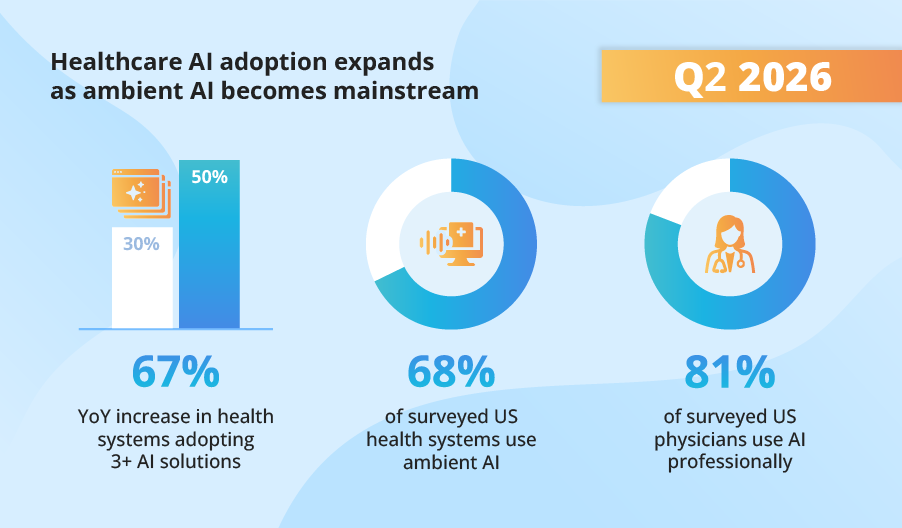
Trend watch
Q2 Healthcare AI Trends by ScienceSoft | July 2026

Gala Batsishcha, MD
Healthcare IT Expert
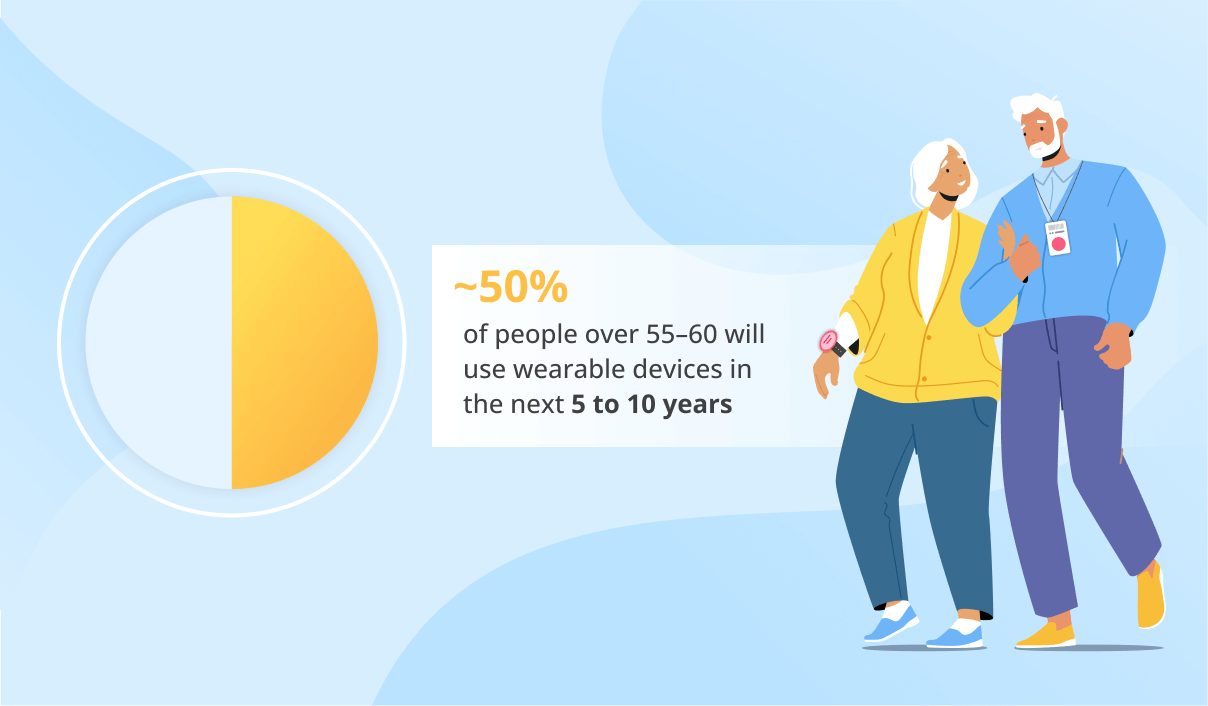
Research
50% of Seniors May Use Wearables As Life-Saving Devices in 2030
Gala Batsishcha, MD
Healthcare IT Expert
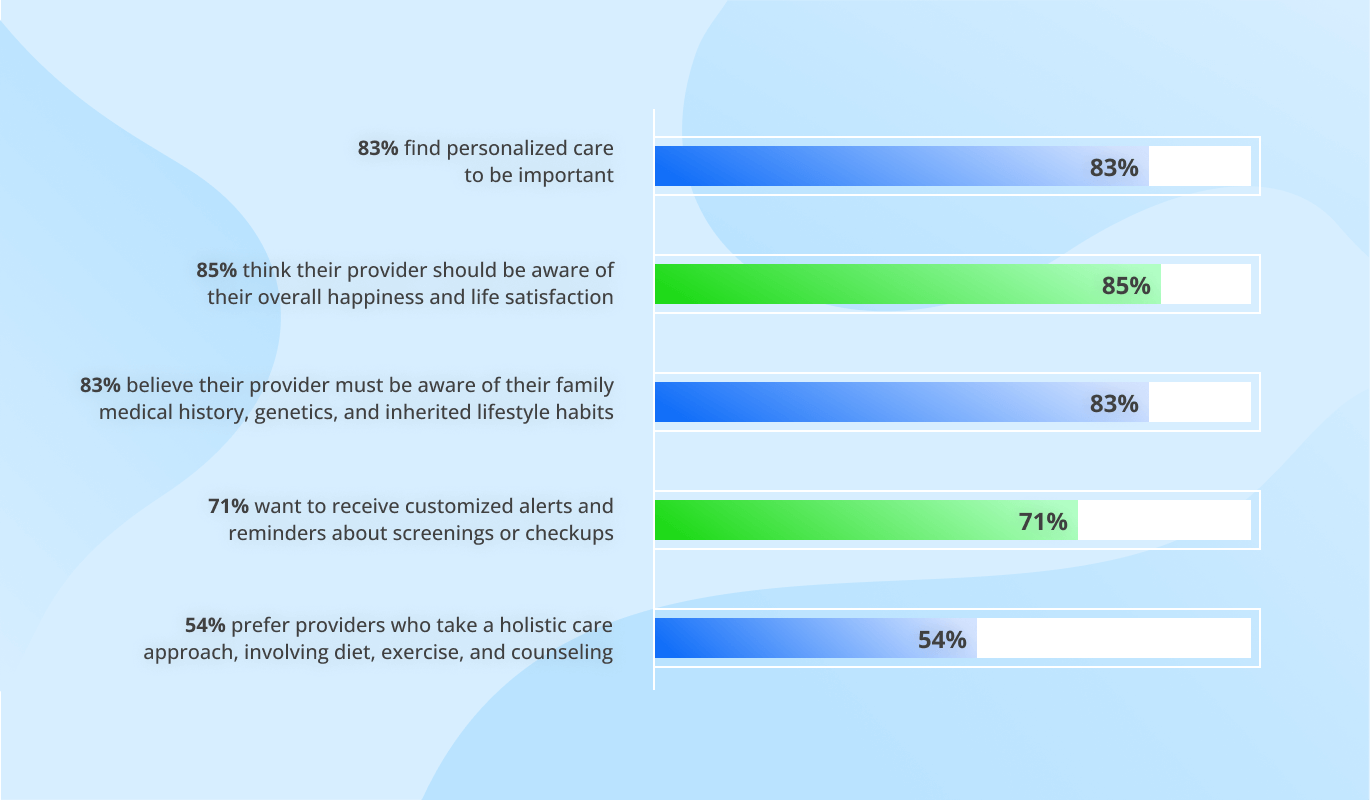
The Power of Personalization in Healthcare With Examples
