EHR for Long-Term Care (LTC)
Capabilities, Integrations, and Development Costs
In healthcare IT since 2005, ScienceSoft designs EHR solutions for SNFs and ALFs that align daily care, reimbursement workflows, and safety programs across facilities and simplify documentation for frontline staff.
 - ScienceSoft")
Contributors

Senior Healthcare IT & AI Consultant, ScienceSoft

Head of AI, Principal Architect, ScienceSoft
EHR for Long-Term Care (LTC) at a Glance
EHR for long-term care provides a shared digital chart that supports long stays, interdisciplinary reviews, and survey-ready records across facilities, backed by pharmacy, lab, and hospital integrations. Advanced platforms may add PDPM optimization, predictive safety and rehospitalization analytics, and AI-assisted documentation to protect reimbursement and reduce clinical workload.
ScienceSoft delivers custom long-term care EHR software as well as targeted LTC EHR modules and extensions for the following skilled nursing facilities and senior care providers:
- Regional SNFs and assisted living groups invest in a chain-wide LTC EHR backbone to replace standard systems that don’t fit specific care pathways, PDPM tactics, and multi-facility reporting.
- Large SNF chains deploy LTC EHR extensions to their existing EHRs to bring together chain-wide safety analytics, rehospitalization control, and PDPM drill-downs in a single cross-facility layer.
- Assisted living and memory care networks implement clinical and safety modules that enhance behavior tracking, fall oversight, and sensor integration beyond what their occupancy-focused senior living platforms support.
Implementation time: 6–12+ months for EHR extension packs and 12–24+ months for a full-scale multi-facility EHR for long-term care.
Development costs: from $250,000 for a targeted LTC EHR extension to $2,500,000+ for an advanced multi-facility platform with SNF reimbursement automation and AI-driven safety and rehospitalization analytics.
Long-Term Care (LTC) EHR Feature Map
Below, ScienceSoft’s consultants present a long-term care EHR feature map that covers most of the clinical, safety, and reimbursement needs of SNFs and long-term care providers we work with. In real projects, clients select and phase in only the functionality that matches their priorities and budget.
Admission, placement, and transfers
![]()
Resident intake and bed management
- Unified resident profiles import data from referral EHRs or portals and consolidate key demographics and coverage to present a consistent chart for clinical and billing teams.
- Payer and coverage snapshots summarize payer mix, benefit periods, and authorizations into one view for quick visibility during intake.
- A bed-and-room-aware census board displays occupancy with isolation status, gender, and payer details to support bed assignment and planning.
- Admission packet automation generates state-specific agreements and consents from templates, routes them for electronic signature, and files them for audits.
Value-adding features:
- A regulatory and clinical pre-admission workspace consolidates PAS and PASRR status, checklists, and approvals to validate incoming residents meet regulatory criteria.
- An intake flow configurator lets multi-facility organizations adjust questions, documents, and placement rules by unit type.
![]()
Care transition and clinical information sharing
- A hospital transition board lists incoming residents with imported discharge summaries, reconciled medications, key alerts, and room readiness indicators for admission planning.
- A care handoff summary generator compiles medications, diagnoses, functional status, risk flags, and recent incidents into structured discharge or transfer packets.
- A clinical results inbox aggregates new lab and imaging results by resident and unit, supports acknowledgment, and links results directly into the chart.
- A hospitalization timeline records each transfer out and return and highlights residents with frequent readmissions.
Value-adding features:
- An external provider collaboration panel shows secure message threads, open questions, and shared tasks with hospital clinicians and payers per resident.
- A readmission review list filters residents with recent hospital stays and opens their timelines and summaries for focused care-transition reviews.
Daily care, medication, and safety management
![]()
Point-of-care documentation on shared devices (workstations, tablets, or handhelds)
- Role-based task lists on point-of-care screens show each CNA, nurse, and therapist their assigned residents and therapy sessions in time order.
- Bedside ADL and vitals charting lets staff record assistance level, intake, and output at the bedside.
- Structured nursing progress notes provide guided templates and flowsheets for long-term conditions and skin status with day-by-day and shift views.
- Multidisciplinary documentation templates capture physical, occupational, and speech therapy, social work, and dietary visits with session duration and type in a single resident chart.
Value-adding features:
- Offline mobile charting stores assignments and recent entries locally during network outages and synchronizes safely when connectivity returns.
- Context-aware point-of-care forms hide irrelevant questions and reuse existing resident data to accelerate completion.
- Bedside monitor connectivity uploads captured vital signs into the resident's chart after a quick wristband scan for patient identification.
![]()
Clinical assessments and interdisciplinary care planning
- A standardized assessment library provides forms for therapy scales and functional assessments (fall and pressure injury risk, pain, cognition, etc.) with scoring and due dates.
- An MDS-focused assessment workspace (for SNFs only) reuses point-of-care and therapy documentation, groups MDS items on one screen, and highlights missing fields for review.
- An interdisciplinary care plan builder turns assessment findings into problems, goals, interventions, and outcomes that therapists, social workers, and dietitians can update in one place.
- A care plan view lists problems, goals, and interventions, as well as recorded incidents, so staff can match documented risks with planned care.
Value-adding features:
- Risk-based care prompts scan assessment scores, vital signs, and resident charts for risk patterns, such as worsening skin status, and flag residents for clinical review.
- Care plan review cycles collect new assessments, incidents, and notes into scheduled review lists with target dates for timely plan updates.
![]()
Medication and treatment management
- Structured order entry forms provide templates and protocol-based suggestions for lab, medication, and treatment orders.
- Drug safety checks monitor allergies, interactions, duplicate therapies, dose ranges, and high-risk psychotropic patterns.
- Med-pass and treatment worklists convert active orders into nurse-specific schedules by resident and time window, highlighting due, overdue, and PRN tasks.
- Unified eMAR and eTAR views let nurses record given, held, and refused medications and treatments with clear reasons.
Value-adding features:
-
A pharmacy integration sends orders to contracted pharmacies, receives dispense data, and feeds antibiotic, vaccine, and other anti-infective use into infection control and stewardship views.
- Controlled substance safeguards support double-witness documentation, shift counts, waste recording, and discrepancy reports for diversion control and compliance evidence.
- Bedside barcode medication checks match resident wristbands and medication packages against active orders.
![]()
Incidents, wounds, and infection control
- A centralized incident log provides forms to record falls, injuries, concerning behaviors, and elopement attempts with linked follow-up tasks.
- A wound and skin care workspace lets teams capture wound stage, size, treatment, and photos at each visit, see wound history in one view, and report healing progress during legal reviews.
- An infection and immunization log provides forms to record infections, antibiotic courses, and vaccination status and displays unit-level exposure metrics to support early cluster detection and antibiotic stewardship reviews.
- A resident safety timeline organizes each resident’s incidents, wounds, and infections into a chronological view for case reviews and care conferences.
Value-adding features:
-
A local fall and behavior trend view summarizes events by resident, unit, and shift to identify high-risk areas and support staffing, routine, or environmental adjustments.
- Survey- and portal-ready documentation packages compile selected incidents, wound notes, photos, and tasks into exportable packets for survey responses, legal reviews, or family portal updates.
Reimbursement, safety analytics, and staffing planning
![]()
Reimbursement and CMS program support (for SNFs and nursing homes)
- A coverage rules engine applies SNF benefit, qualifying, and authorization rules during admission and stay updates to identify non-covered days and approval gaps.
- A PDPM case mix and rate view translates MDS items, functional scores, diagnoses, and therapy patterns into PDPM groups and expected daily reimbursement rates per resident.
- An MDS submission workspace builds export files from completed assessments, runs current CMS edit checks, and displays accept or reject statuses.
- An SNF claim file builder assembles institutional claims with PDPM rates, covered days, and occurrence codes for export to existing billing systems.
Value-adding features:
- A denial and underpayment tracker imports payer responses, groups recurring denial reasons, and links them to MDS and coverage rules to support corrective actions.
- A regulatory content manager stores PDPM, MDS, and coverage rule sets with effective dates to maintain consistent reimbursement logic across facilities.
![]()
Safety, rehospitalization, and staffing analytics
- Clinical safety dashboards combine unit-level census, incidents, wounds, infections, antibiotic and psychotropic use, and documentation gaps to support daily safety oversight and stewardship reviews.
- A rehospitalization and deterioration risk panel ranks residents by near-term transfer risk and groups recent warning signs for case-review huddles.
- Fall and behavior risk views overlay fall risk scores, recent events, and safeguards in place by location to highlight high-risk units.
- A staffing optimization board combines census and basic acuity data to determine recommended staffing levels for each unit.
Value-adding features:
-
A calculator for quality measures and Five-Star score (for SNFs only) computes CMS metrics from MDS responses and clinical data and links each measure to residents and documentation.
- A survey risk and correction plan workspace displays unit-level incidents, prior regulatory deficiency tags, and quality measures, along with the corrective action tracker.
AI Tools for Long-Term Care EHR: Popular Use Cases
ScienceSoft helps long-term care providers implement secure, transparent AI tools that automate documentation, make PDPM and survey work more predictable, and identify residents at risk early. The benefits in the examples below are indicative only and depend on data quality, workflow maturity, staff adoption, and governance. ScienceSoft recommends validating impact in a short pilot with clear baseline metrics before scaling.
Each scenario below can be implemented as clinician-in-the-loop decision support, so staff can see key inputs, adjust thresholds, and override suggestions, drawing on FDA Clinical Decision Support guidance and ONC HTI-1 transparency principles where they apply.
We typically deploy these tools on HIPAA-compliant cloud infrastructure with end-to-end encryption, RBAC, audit logging, and bias checks to help providers address CMS nursing home expectations and ACA Section 1557 nondiscrimination rules without adding extra compliance overhead.
![]()
AI-assisted clinical documentation and care planning
Ambient AI tools can capture bedside conversations and convert them into draft nursing notes, ADL records, and incident reports. LLM assistants can structure free text into MDS-aligned fields, summarize recent documentation, or suggest prefilled care plan text for the clinician’s review.
Reported benefits: up to 50% less time spent on documentation reported with ambient AI tools.
![]()
AI copilot for clinical, MDS, and regulatory tasks
An AI copilot can generate resident, unit, and shift summaries to support rounding, handoffs, and safety reviews. Such tools can support MDS and PDPM “what-if” analysis for coding decisions and draft regulatory narratives for surveys, QAPI reporting, and board communications.
Reported benefits: ~30% less chart review burden with AI assistants.
![]()
Predictive AI for rehospitalization and deterioration risk management
Predictive models can calculate near-term rehospitalization and deterioration risk scores from diagnoses, vitals, ADLs, and MDS data. They can flag higher-risk residents for care team review, show which inputs drove each score, and support early warning sign detection.
Reported benefits: ~10–15% fewer 30-day readmissions in AI-supported risk control programs.
![]()
AI assistant for acuity-driven nurse staffing
Staffing AI tools can combine census, acuity data, and regulatory rules to estimate required nurse hours and test staffing scenarios. They can draft balanced rosters as well as suggest reassignments or call-ins when acuity spikes or shifts are dropped.
Reported benefits: up to 70–80% less manager time on schedule-building in healthcare AI staffing programs.

What Makes AI Scribes Practical
In this interview, Hadeel Abu Baker examines where AI medical scribes help most, and what limits their safe use. It is a strong fit for long-term care EHRs that convert bedside conversations into draft notes, ADL records, and incident reports.

Shape Your EHR Roadmap With ScienceSoft
Important Integrations for Long-Term Care (LTC) EHR
In EHR systems for long-term care, reliable integrations with hospital records, labs, CMS, and revenue systems often determine whether providers can avoid claim leakage, survey issues, and staff hours lost to retyping. ScienceSoft handles this at the architecture level, using patterns recommended in the ONC ISA and other industry best practices.
In full-scale builds, ScienceSoft defines a canonical clinical and billing data model and connects partner systems via HL7 or FHIR for clinical data, NCPDP for pharmacy, and X12 for eligibility and claims. When a non-interoperable EHR remains in place, we add an integration layer that maps the EHR’s data to the canonical model and exposes standardized file formats or APIs, so providers can connect with partners without double-entry or creating new custom integrations each time.
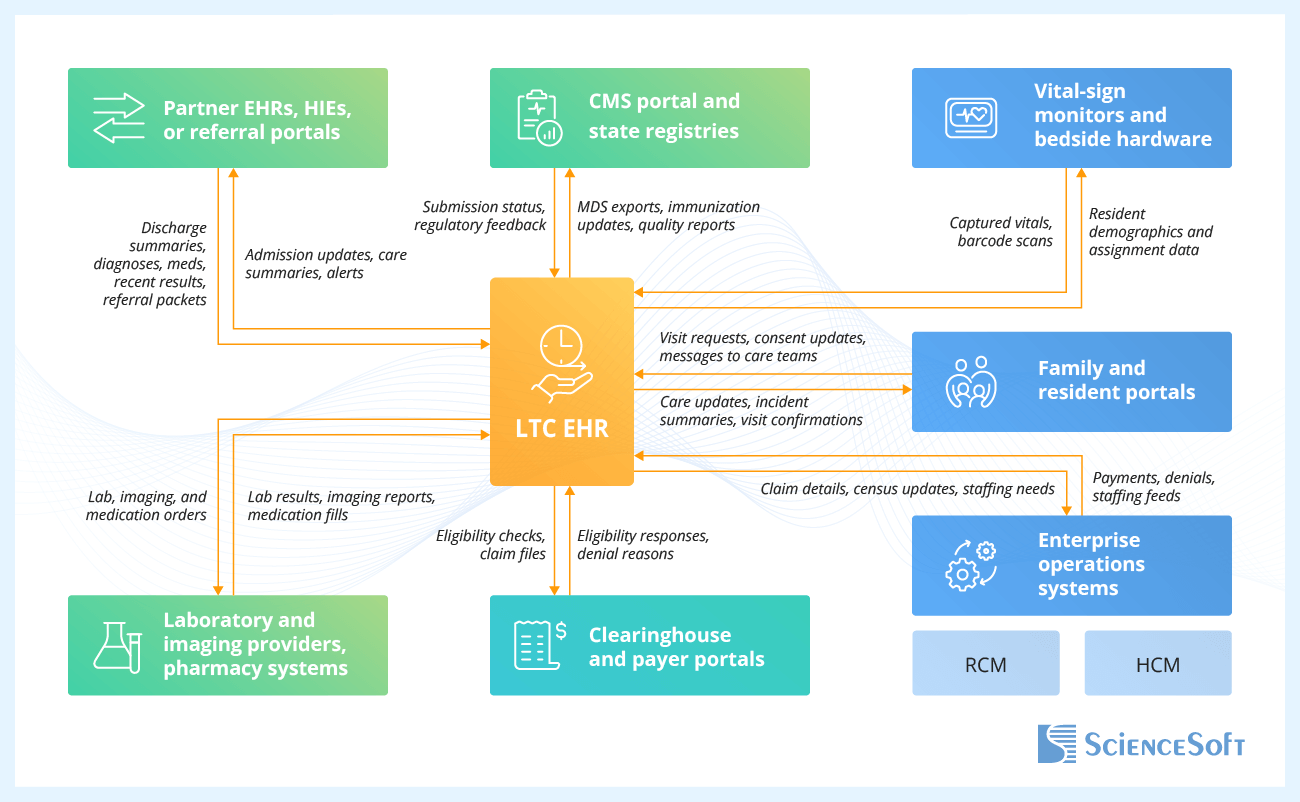
- Hospital EHRs, HIEs, and referral portals — to pull discharge summaries, medication lists, diagnoses, and recent test results straight into admission workflows; to send admission notices and care summaries back when residents transfer.
- Laboratory systems, imaging provider systems, and pharmacy software — to send lab, imaging, and medication orders from the EHR and receive results and fills that update eMAR, infection tracking, and stewardship metrics.
- Family and resident portals — to share near-real-time care updates, incident summaries, and visit schedules with families, and to collect digital consents into the resident chart.
- Revenue cycle management (RCM) system — to export LTC claim data, PDPM rates, and census updates from the EHR, and to import payments and denials that feed posting, analytics, and payer dashboards.
- CMS portal and state registries — to submit MDS, quality measure, and immunization data from the EHR and receive status, error messages, and scores that guide survey preparation and QAPI priorities.
Other frequently requested LTC integrations include single sign-on services, HR and scheduling systems, document scanning tools, and nurse call and safety sensor platforms that centralize alerts and content in the EHR.
Development Tips for Long-Term Care EHR Projects
Below, ScienceSoft’s experts identify three development areas that often lie at the root of common problems LTC providers face with their EHR systems. For each one, we describe engineering practices our teams rely on to keep these platforms’ parts predictable.
![]()
PDPM and MDS as a rule engine, not screen code
In EHR systems for SNFs and nursing homes, PDPM and MDS rules should live in a versioned engine that assessment screens and claim builders call through stable APIs. This way, when CMS guidance changes, IT teams can update rules and rerun automated regression tests using reference residents, rather than editing dozens of forms and reports. This keeps PDPM groups, per diem rates, and quality metrics aligned across facilities even during busy regulatory cycles.
![]()
eMAR performance shaped around peak med rounds
Stable LTC eMAR deployments start with clear written performance goals for peak med rounds that cover response time, sync frequency, and error handling. If those targets are not agreed upon up front, problems like slow screens, stuck syncs, or lost offline entries usually show up only after nurses lose trust in the system. ScienceSoft links this performance agreement to automated load tests and easy-to-read live metrics, so operations staff can see med pass performance in real time.
![]()
Analytics-ready LTC event model and governed metrics
LTC EHR gains more value when daily EHR records feed an event data layer that stores each incident, vital, medication administration, and reimbursement change with resident, unit, and time tags. Without this model, each report pulls from its own mix of tables, exports, and manually edited files, so the same measure is counted in different ways. For example, multi-site providers then see QAPI packs, PDPM reviews, and board reports use different numbers for one period. This weakens trust in analytics, AI output, and internal benchmarking. ScienceSoft defines metrics in this dedicated event layer and adds simple checks, so executives and clinical leaders can work with one trusted set of numbers.
Some LTC EHR modules can be built more economically with low-code tools such as Microsoft Power Apps. For example, you can use Power Apps to build back-office safety and compliance workflows, such as an incident and infection hub with chain-wide safety views and survey-ready documentation packs. Beyond faster rollout, low-code modules also let you make manual tweaks to the software logic when regulations change, often without software developers.
However, it’s important to remember the limitations. When heavy image volumes, offline use, and complex analytics are needed, Power Apps alone may not be enough, so providers still need custom code, separate storage, or reporting layers.
How Much Does It Cost to Develop EHR for Long-Term Care?
The cost of long-term care EHR development typically ranges from $350,000 for focused clinical or safety modules to over $2,500,000 for a full-scale multi-facility platform.
The project budget will depend on the number of communities in scope, the depth of clinical and reimbursement features, the complexity of integrations, and the extent of AI and analytics you plan to introduce.
The options below outline scope bundles and corresponding cost ranges that cover the most common needs of our long-term care clients.
|
|
Clinical and safety LTC EHR module |
LTC EHR extension pack |
Full-scale LTC EHR build |
|---|---|---|---|
|
Best for
|
Assisted living and memory care networks that prioritize safety controls, behavior tracking, and fall reduction. |
SNF chains that need to enhance chain-wide PDPM, rehospitalization, and safety analytics in their existing EHRs. |
SNFs and assisted living groups that want a single clinical and reimbursement backbone across facilities. |
|
Standard functionality / Common extension types
|
$250,000–$800,000 |
$350,000–$900,000 |
$700,000–$1,400,000 |
|
Advanced functionality
|
$750,000–$1,500,000+ |
$900,000–$1,800,000+ |
$1,400,000–$2,500,000+ |
Why Choose ScienceSoft as Your EHR Development Partner
- Since 2005 in healthcare software engineering and IT consulting.
- 150+ successful projects in the domain.
- Architecture and Solutions CoE to design secure, integration-first solutions with offline-tolerant point-of-care features and canonical data models for legacy-heavy environments.
- Proficiency in aligning healthcare software with HIPAA, GDPR, CMS nursing home regulations, and the 21st Century Cures Act.
- Expertise in data exchange standards, including HL7 v2, FHIR, C-CDA, USCDI, NCPDP, and X12; clinical coding standards, such as ICD-10-CM, SNOMED CT, and LOINC; and QRDA/MDS-based quality reporting.
Certifications and awards
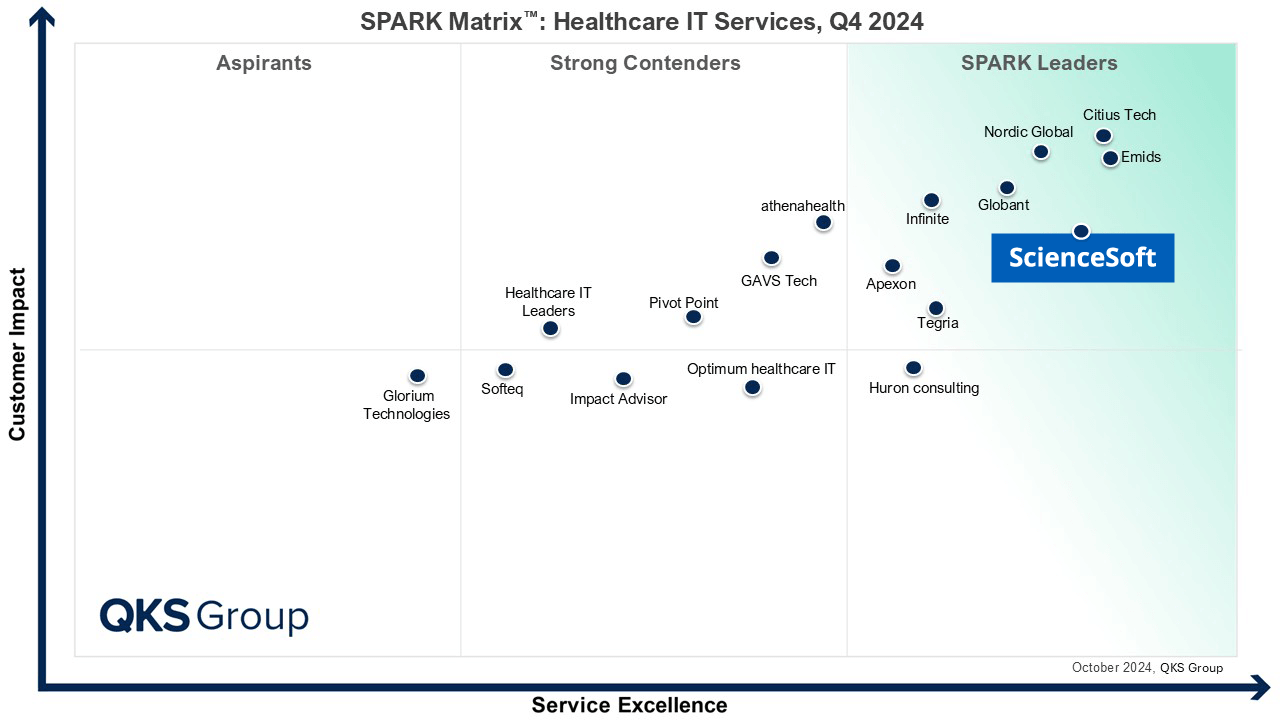
Featured among Healthcare IT Services Leaders in the 2022 and 2024 SPARK Matrix

Recognized for Healthcare Technology Leadership by Frost & Sullivan in 2023 and 2025
Named among America’s Fastest-Growing Companies by Financial Times, 5 years in a row
Top Healthcare IT Developer and Advisor by Black Book™ survey 2023

Four-time finalist across HTN Awards programs

Named to The Healthcare Technology Report’s Top 25 Healthcare Software Companies of 2025

HIMSS Gold member advancing digital healthcare

ISO 13485-certified quality management system

ISO 27001-certified security management system
What Our Healthcare Clients Say

Our project required a large amount of industry-specific methodology and algorithms to be implemented into our new software connected to EHR/LIS systems, which the team handled well. ScienceSoft has been a competent partner for medical software development. They are reliable, thorough, smart, available, extremely good communicators, and very friendly.

Our clients in healthcare rely on Qventive for the support and administration of essential software solutions such as EHR and practice management systems. The transition phase only lasted a couple of weeks: ScienceSoft’s team quickly adapted to our processes and understood our clients’ expectations from the start, which made things a lot easier for us. We appreciate their proactive communication and commitment to quality.

During our cooperation, ScienceSoft proved to have vast expertise in the Healthcare and Life Science industries related to the development of desktop software connected to laboratory equipment, a mobile application, and a data analytics platform. They bring top-quality talents and deep knowledge of IT technologies and approaches in accordance with ISO13485 and IEC62304 standards. I would also like to point out that ScienceSoft’s team demonstrated a great engineering culture, a proactive approach to work, and the communication was easy and clear.

I honestly can’t say enough about how impressed I am with ScienceSoft. They delivered a fully customized AI medical chatbot PoC in just two weeks, which was unbelievable. The attention to detail in the chatbot design, and especially the pitch deck, was amazing — with this kit on hand, we are ready to go into investor discussions confidently. It’s not often that you find a team that moves this fast without sacrificing quality. I’m genuinely grateful to ScienceSoft for their hard work and would absolutely recommend them to anyone looking for top-notch results in health tech.
